



GSB orthodontic
※ GSB orthodontic(Seoul, Korea)
Dr. Jinhaeng Lee (Board Certified Orthodontist)
Inventor of MCB technique and MCB splint.
2021 Marquis Who's Who in the World.
2020 Marquis Who's Who in the World.
2020 Wynn Who's Who in the World
2019 Marquis Who's Who Top Doctor
2017/2018 Marquis Who’s Who in the World
2017/2018 Albert Nelson Marquis Lifetime Achievement Award.
2018 Industry leader with Marquis Who’s Who Top Professional Series.
https://www.facebook.com/jinhaeng.lee.125
https://www.facebook.com/gsbortho/
http://3.39.27.217/
----------------------------------------------------------------------------------------------------------------
※ Why does my body change over time?
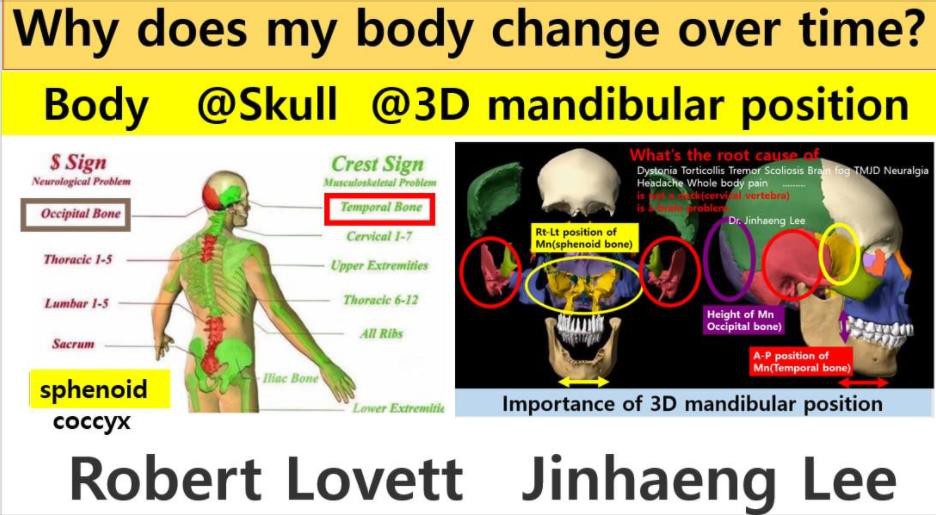

Why does my body change over time?
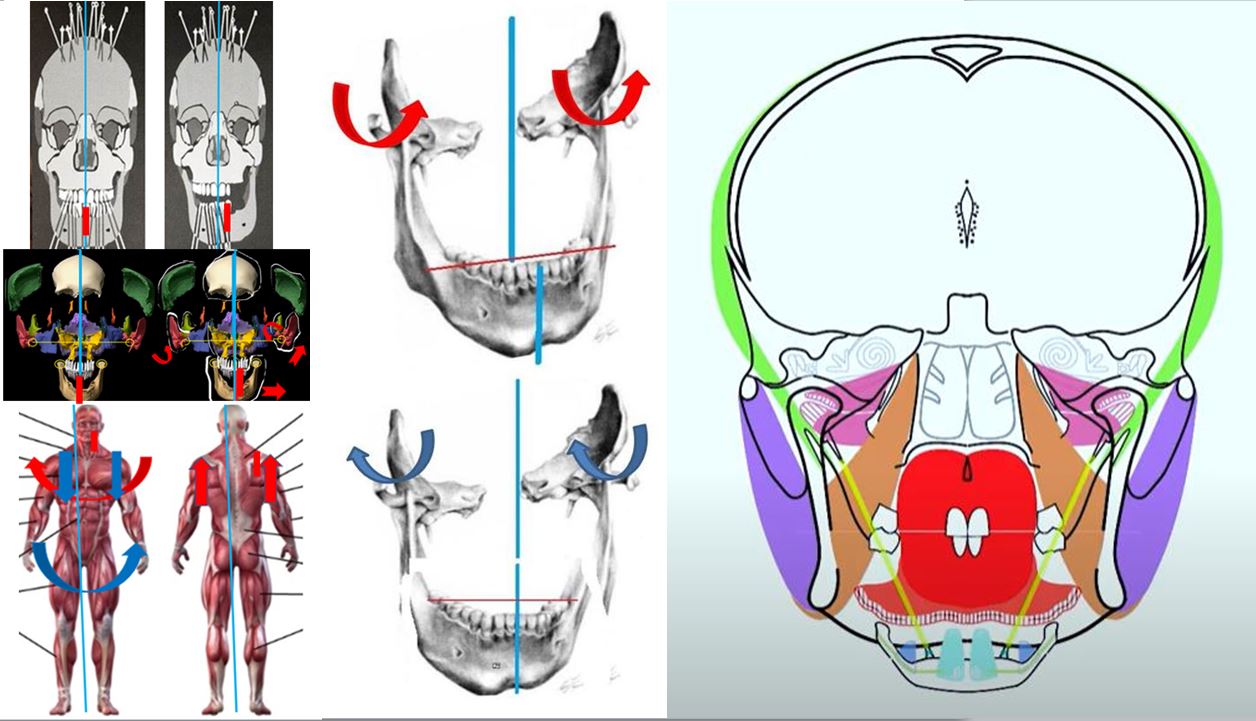
Back at the beginning of the twentieth century, orthopedist Robert Lovett described in his works the relationship in the human skeletal structure in the S shape and in the # shape, in which the occipital bone correlates with the thoracic spine (T1-5), lumbar and sacrum, and the temporal bones correlate with cervical spine (C1-6), shoulder blades, ribs, thoracic spine (T6-12) and pelvic bones. Therefore, any change in the spatial position of the occipital bone leads to changes in the position of the upper thoracic and lumbar spine and sacrum (however, there is also reverse connection), and the asymmetric rotation of the temporal bones in the skull will always occur simultaneously with the asymmetric rotation of the pelvic (iliac) bones, i.e. synchronously, but in a mirror image, as well as changes in the cervical and lower thoracic spine.
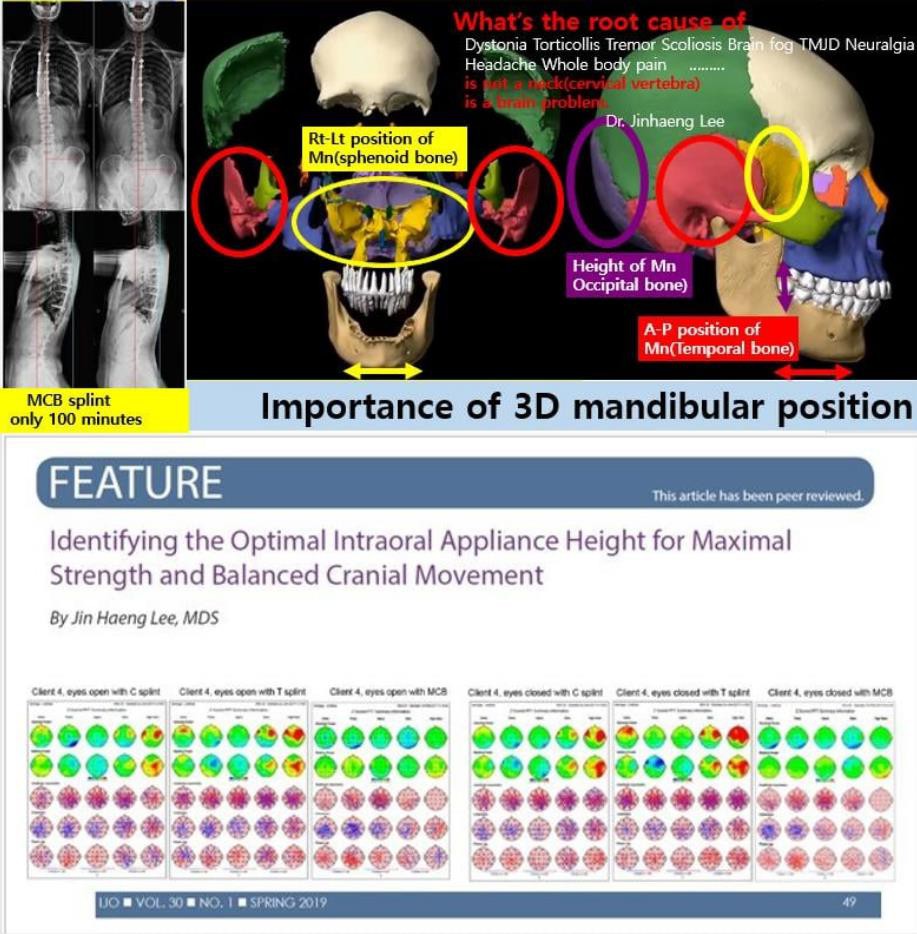
Dr. Jinhaeng Lee first posted on Facebook on September 5, 2020 how the three-dimensional position of the lower jaw relates to the skull.
I found that the related bone distortion coincided with the distorted direction of the sphenoid temporal occipital bone, and when the MCB splint was worn, it was confirmed by the palpation of the finger that the direction was changed in the opposite direction.
If someone has symptoms such as a distorted body, pain, lack of strength, or tremor etc, I recommend that you first be diagnosed with a osteopathic doctor(D.O). If the osteopathic doctor says your symptoms get worse when you touch your teeth, those symptoms can be treated a splint(MCB splint) that places the lower jaw in a position where the head bone gets better and osteopathy.
Can your splint keep your body from leaning forward?
The MCB splint is manufactured to promote the movement of the sphenoid, temporal, and occipital bones. When wearing this MCB splint, all skull bones move in the opposite direction without twisting. Then, all the muscles in your body will start moving upwards instead of downwards. If the splint you're wearing is neurologically effective, it should move all the muscles upward. No matter what kind of splint you make, if you can't get all of your muscles to move upward, that splint is not moving your skull normally.
------------------------------------------------------------------------------------------------------------------------------------------
CLINICAL ASPECTS OF THE CRI (Cranial Rhythm Impulse) and mcbsplint
The rate of the CRI decreases in a variety of conditions, for example, psychological disturbances, 11 traumatic brain injuries,31and in neonates after a difficult birth.32 Low CRI rates have also been reported in patients who are comatose14 and in children with developmental delays .14, 3 3 Anecdotal reports suggest that the CRI also decreases in other circumstances, for example, emotional exhaustion, malnutrition, metastasis,14 and many other maladies. The CRI rate is increased in patients who have acutefever12 and in hyperkinetic and autistic children.14
The CRI amplitude must also be assessed; this quality is more difficult to appraise than the rate. Low CRI amplitude has been variously described as a palpable sensation of low volume12and as a labored, low-energy, or lethargic effort.14 Excess amplitude has been characterized as “the profound repercussion of a wave striking a rock-bound coast”12 and as a wave “in a rigid container fighting against its boundaries.”14
CRI fluctuations should be bilaterally symmetrical,1 2, 14 even though many body rhythms are lateralized, with the left and right sides oscillating in different phases.3 4 Nonsymmetrical CRI findings are interpreted as signs of restrictions in the articulations in the cranial sutures or as membranous tension within the intracranial falx cerebri, falx cerebelli, and paired tentoria.1 2 , 14 Besides its use in the diagnosis, the CRI also provides a fulcrum for a treat in restrictions in cranial bones and fascial membranes. Treatment is accomplished by following sensed CRI motion with the hands (in any direction on — broadening, narrowing, flexion, extension, torsion, and so forth) and then either exaggerating the motion or resisting it.3 5 This treatment seems to balance the movement and make the motion symmetrical.
The mcb splint affects the rate, amplitude, and bilateral symmetrical fluctuation of CRI and the rhythm of the whole body moves in a balanced way.
So, as soon as you wear the mcb splint, all the twisted bones begin to level, and all the muscles that have fallen down are lifted up, making your body less tiring and stronger. If orthodontic treatment is performed at the position of the lower jaw at the mcb position, it will get better every time the teeth touch for the rest of your life.
The way humans live healthily is through the bones of the skull to improve movement. Isn't this the Bulloch(herb of eternal youth) that King Jinshi(Qin Shi Huang) looking for?
*Walter C, Lechner KH, Karl M. A pilot study on spatial changes in the maxilla caused by osteopathic therapy. Quintessence Int. 2015 Jan; 46(1):81-6. PS
A variety of theories on the pathogenesis of temporomandibular disorders (TMD) exists resulting in treatment approaches ranging from the fabrication of occlusal splints to alternative treatment modalities such as osteopathy. The goal of this pilot study was to investigate whether osteopathic treatment causes spatial changes in the maxilla.
Following ethics commission approval and informed patient consent, three patients diagnosed with TMD participated in this investigation. In addition to regular treatment, an individualized mandibular occlusal splint was fabricated and a maxillary silicone impression was made.
Following osteopathic treatment, the splint was adapted intraorally and another maxillary impression was made. Before and after treatment, the splint and the impressions were scanned three-dimensionally. The resulting images were superimposed using best-fit matching algorithms.
Inconsistent spatial changes in the posterior areas were observed both in the maxillary impressions as well as in the mandibular splints reaching maximum absolute values of 0.50mm.
Based on this pilot study, it appears that osteopathic treatment may be capable of inducing spatial changes in the maxilla due to sutural movement thereby validating the fundamental principles of osteopathic treatment.
Although based on the study conducted, it cannot be concluded that osteopathy constitutes a successful treatment alternative in TMD patients, practitioners should be aware of this treatment modality.
------------------------------------------------------------------------------------------------------------------------------------------

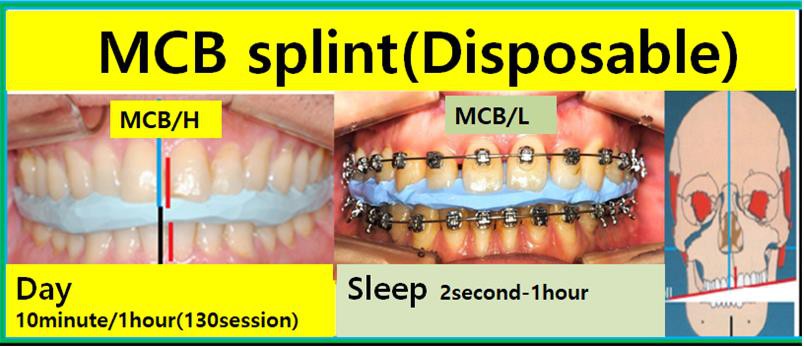
※ There are two types of MCB splints:
1. MCB/H (High)
The first type is a disposable splint used for 10 minutes, and it is employed in MCB techniques. This splint is highly effective in coordinating all the movements of the skull.
For example, a nurse patient underwent 8 hours of laparoscopic surgery for uterine fibroids and was given 7 days of sick leave for recovery at the hospital. When wearing this splint, the mobility of the surgical site gradually decreased, making the patient more comfortable, and the surgical site began to heal. Initially, the effect lasted for 10 minutes.
In the case of dystonia patients, the splint immediately corrects the twisted posture, allowing the head to straighten. However, symptoms reappear after 10 minutes. Therefore, after checking the incorrect direction, the splint is remade and worn again. As the treatment progresses, the patient's symptoms gradually improve according to the degree of skull distortion. However, the treatment time extends to 1 hour after approximately 130 sessions. It is also observed that the overall body distortion improves through palpation.
2. MCB/L (Low)
The second type is a low-profile disposable splint. This splint is worn at bedtime and is thinner than the MCB/H device used during the day. The characteristic of this device is that it is worn during sleep, allowing for a relatively long period of effectiveness. When the skull's movement becomes distorted, the splint is remade and worn again. During orthodontic treatment, the final thickness is adjusted so that the MIP (maximum intercuspal position) is 0mm in the front, back, left, and right positions. For dentures or full-mouth prostheses, the teeth are treated to achieve MIP at 0mm. When the teeth occlude in this position, the patient's skull moves normally every time the teeth touch, and overall health improves over time. This position is relatively easy to find.
3. Teeth Contact Position (Maximum Intercuspal Contact Position)
This is the position used when treating malocclusion with orthodontic treatment.
Currently, most orthodontic treatments involve moving teeth while they are in contact. If the left and right centers of the lower jaw are misaligned after correction is completed, the sphenoid bone will continue to shift and move. If the lower jaw is not centered anteroposteriorly, the temporal bone will shift and move. Ultimately, if the height of the teeth is off when they occlude, the occipital bone will become misaligned. If the occlusal height is low, the left occipital bone continues to signal misalignment, but if the dentist cannot palpate it, the patient may not be aware. However, over time, these effects gradually begin to appear in the body. Therefore, if you undergo orthodontic treatment, your teeth must be aligned in the three-dimensional position of the lower jaw that normalizes the movement of the skull.
Then, your teeth will serve as an MCB splint for the rest of your life, normalizing the movement of the skull every time they touch. Could this be the herb of immortality that Emperor Qin Shi Huang sought?
------------------------------------------------------------------------------------------------------------------------------------------
Symptoms that can be treated with MCB splint:
Cranial Osteopathy by MCB (mabdibular cranial balancing) splint.
Cranial/Postural distortion.
Extraction Orthodontic Reversal. MARPE. ALF. Dystonia. Brain Fog.
Neuralgia. Scoliosis. Tremor. TMJ Disorder. Facial Pain.
Neurological Symptoms. Headache. Visual disturbance. Head
surgery or injury disturbance. Functional disturbance of the brain.
Vertigo. Hearing and balance disturbance. Insomnia.
Psychological disturbances. Tic disease. Tourette syndrome.
Sleep apnea syndrome.Dizziness. Ear ringing. Nose breathing
disorder. Chest hump. Eye asymmetry. Cranial problems. Ear
asymmetry. Cheekbone asymmetry. One side crumbled face.
Lower back pain. Gastrointestinal problems. Excessive gastric acid.
Abdominal swelling. Displaced pelvis. Pelvic distortion.
Continuous feeling of wanting to urinate. Spine problems. Panic
disorder. Sleep disorder. Insomnia. It is recommended to receive
mcb splint treatment before any surgery. etc
------------------------------------------------------------------------------------------------------------------------------------------
$Price
*If you visit South Korea with a 90-day tourist visa, the only treatment available is the MCB splint treatment.
MCB splint treatment is the most effective treatment method for those with a valid 3-month visa.
*Please bring any devices or splints you have previously received.
*If you have copies of your CBCT or MRI, please email them to us in advance.
*If you have severe scoliosis or kyphosis, a full-body X-ray will be required. (This will be done at another hospital.)
*Please fill out the questionnaire, and we will take your photos and basic X-rays at our dental clinic.
*To create the MCB splint (made of resin), we will scan your upper and lower jaws at our clinic.
*To increase the treatment effect in a short period, about 15 MCB/Hs should be made daily (initially, an MCB/H should be made every 10 minutes). Our clinic can produce about 10-20 MCB devices per day on Mondays, Tuesdays, Thursdays, Fridays, and Saturdays (this is possible only if there aren't many patients).
*Our clinic is closed every Wednesday. We recommend receiving full-body treatment with osteopathy on Wednesdays when the clinic is closed.
*Typically, after at least 130 sessions of MCB/H treatment, the movement of the skull does not change for an hour. From this point on, the patient should make a device every hour, allowing for about 5 MCB/Hs to be made daily.
*The more MCB/L devices are made, the longer the patient will need to wear them. When MCB/L is first made, the effect lasts for less than 2 minutes, so the more MCB/Ls are made, the effect can extend from 2 minutes to 1 hour.
https://g.co/kgs/5HmZ9M
♡ Jaw Joint Treatment Fee (As of December 15, 2023)
※ Iteroscan & Panoramic & Cephalometric & PA/ 150,000 KRW // 300,000 KRW CT is the next day.
※ MCB treatment fees are subject to change.
Auxiliary Devices
Customized Splint (device made of dental resin/thermosplint) ---------------------- 700,000 KRW
Splint Adjustment Cost / 50,000 KRW
MCB Treatment Fee (Disposable Device)
1 Session 100,000 KRW
30 Sessions 2,100,000 KRW
50 Sessions 3,500,000 KRW (+5 Sessions/Total 55 Sessions)
100 Sessions 7,000,000 KRW (+15 Sessions/Total 115 Sessions)
★ 10,000,000 KRW per day per person (10am-6pm/lunch break 1-2 pm)
---Treatment fees are subject to change----
★ MCB splint improves head bone movement and corrects the alignment of the jaw joints, face, and head bones. This is a natural treatment based on the body's self-healing mechanism, and if treated multiple times during a short visit, it will increase the treatment effect and shorten the treatment period.
★ If the package treatment is discontinued, you will need to pay 100,000 KRW per session.
To create a 400-session MCB splint:
If the device's effect lasts for 10 minutes, 15 sessions per day should be done over 8.7 days (5 hours of treatment time are required in the hospital).
After 130 sessions, the device's effect lasts for 1 hour, so if treated 5 times a day (6 hours of treatment time are required in the hospital), it takes 54 days to complete the remaining 270 sessions.
To follow this schedule, you must receive MCB treatment at the hospital for at least 70-80 days and adjust your schedule accordingly.
*Invisalign Treatment Fee 7,000,000 KRW
-----------------------------------------------------------------------------------------------------------------------------------------
Is it possible to treat mandibular asymmetry without surgery?
It is currently known that the lower jaw cannot move without surgery.
Most orthodontic treatments correct teeth based on the current occlusal state.
In orthodontics, the temporal bone connected to the lower jaw is taught to be an immovable bone.
However, in 1974, American osteopath Dr. Magoun wrote in the Journal of Osteopathic Medicine (Journal AOA/vol. 78, June) that the fundamental cause of mandibular asymmetry lies in the misaligned temporal bone.
He stated that the left temporal bone is in external rotation while the right is in internal rotation, causing the midline of the lower jaw to shift to the left, resulting in misaligned teeth.
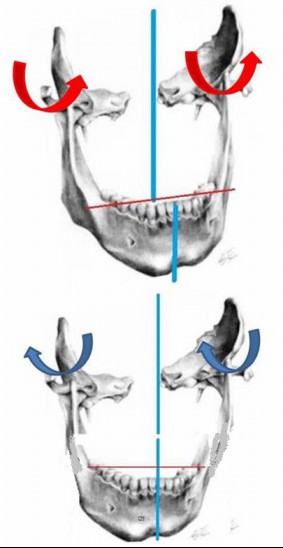
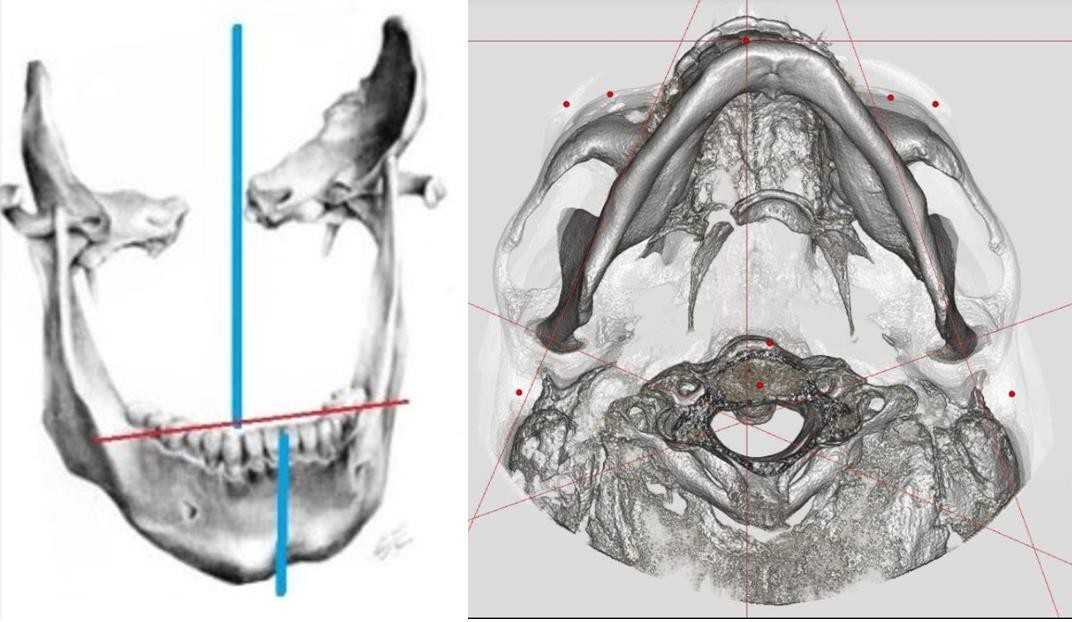
So, if we move the center of the lower jaw to the center of the face, will the temporal bone move?
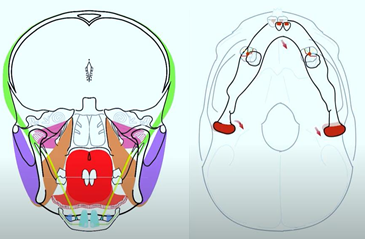
The lower jaw is directly connected to the temporal bone (light green/purple).
If the center of the lower jaw is moved to the center of the face,
it can be observed that the temporal bone moves quickly as a result.
Additionally, the lower jaw is directly connected to the sphenoid bone (orange/light green), causing the sphenoid bone to move as well.
In other words, if the lower jaw is misaligned, the temporal bone, sphenoid bone, and occipital bone (indirectly connected) are also misaligned.
This is because the muscles continue to pull in an unbalanced manner.
-----------------------------------------------------------------------------------------------------------------------------------------
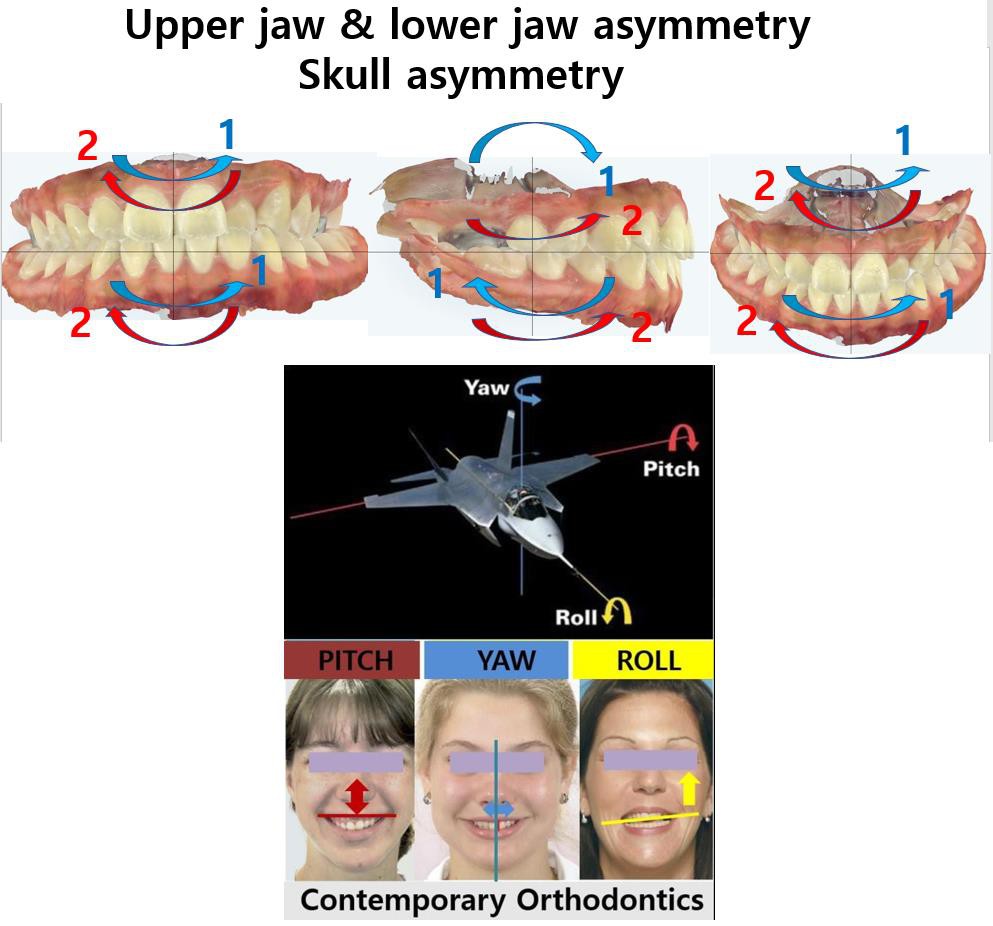
The misalignment of the upper and lower jaws is something that all humans possess.
This misalignment fundamentally originates from the misalignment of the cranial bones.
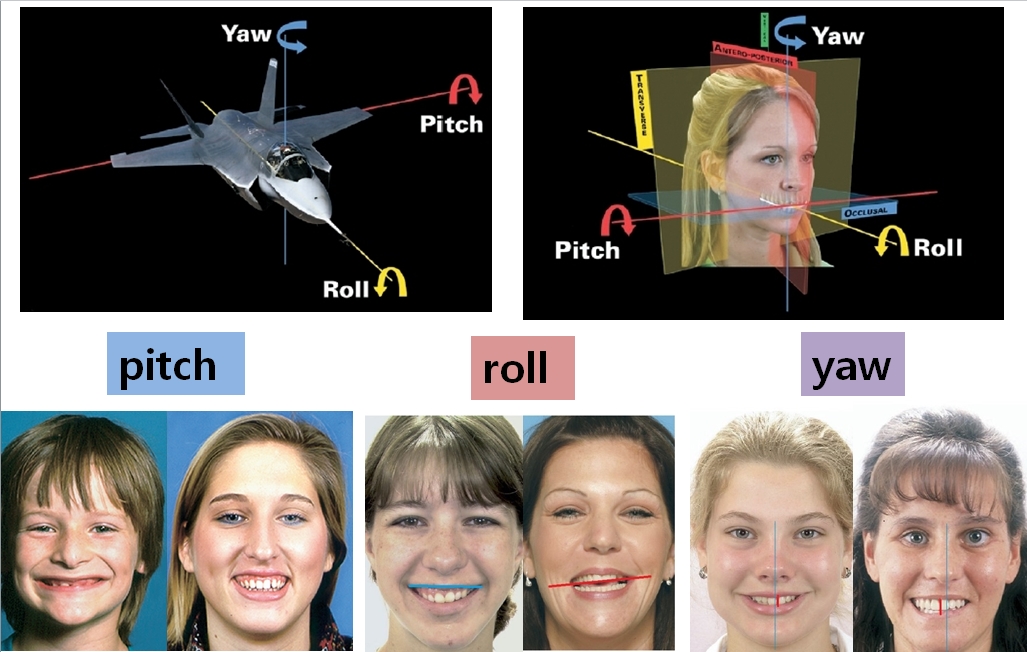
The distortion of the face in frontal, lateral, and transverse planes causes the bones to shift in those distorted directions every time the teeth make contact.
This distortion affects the cranial nervous system, continuously causing the face and body to become more misaligned.
However, there is a specific position where such distortion does not occur. When the teeth make contact in this position, the misaligned bones rotate in the opposite direction, causing facial wrinkles to smooth out and the body to straighten.
This position is called the MCB (mandibular cranial balancing) position. During any orthodontic treatment, teeth should be moved so that they occlude in this position. The movement of the misaligned upper and lower jaws can be more easily treated with Invisalign compared to traditional bracket orthodontics. When the teeth contact in this MCB position, it generates strength in all the muscles because the misaligned structures are corrected and realigned.
These principles apply equally to splint therapy.
For example, in cases where anterior open bite occurs during splint therapy. The cause of the open bite is due to the maxilla and mandible being pitched backward. If this natural movement is not understood and the splint is adjusted incorrectly, the mandible will continue to move backward, causing the face to become misaligned.
This will result in an anterior open bite.
If, after splint therapy, the patient experiences less strength when their teeth are in contact compared to when their mouth is open and the teeth are not touching, it means that the position of the mandible is misaligned.

As shown in the image, when the teeth occlude in the correct position of the mandible, the misaligned facial bones move in the opposite direction, and the twisted shoulders and pelvis also move in the opposite direction. This is proven by the fact that when the teeth come into contact, strength is generated throughout the body.
However, if the mandible is in a misaligned position, the strength will weaken when the teeth come into contact.
Is your mandible in a good position? If the strength weakens when your teeth come into contact, you should only allow your teeth to touch while eating. If you grind or clench your teeth, your face and body will continue to twist.
-----------------------------------------------------------------------------------------------------------------------------------------
It has been 27 years since Invisalign orthodontic treatment was introduced.
Now, the era of Invisalign, which only corrects teeth, is over.
While correcting the misalignment of teeth, the distortion of the face should also be improved.
To do this, orthodontists must understand facial distortion.
If treatment is done without this knowledge, the distortion of the face and body may worsen.
During Invisalign treatment, it is possible to create a treatment plan to improve facial distortion.
When the Invisalign device made in this way is worn, the distorted face moves in the opposite direction, and the misaligned body also begins to move correctly.
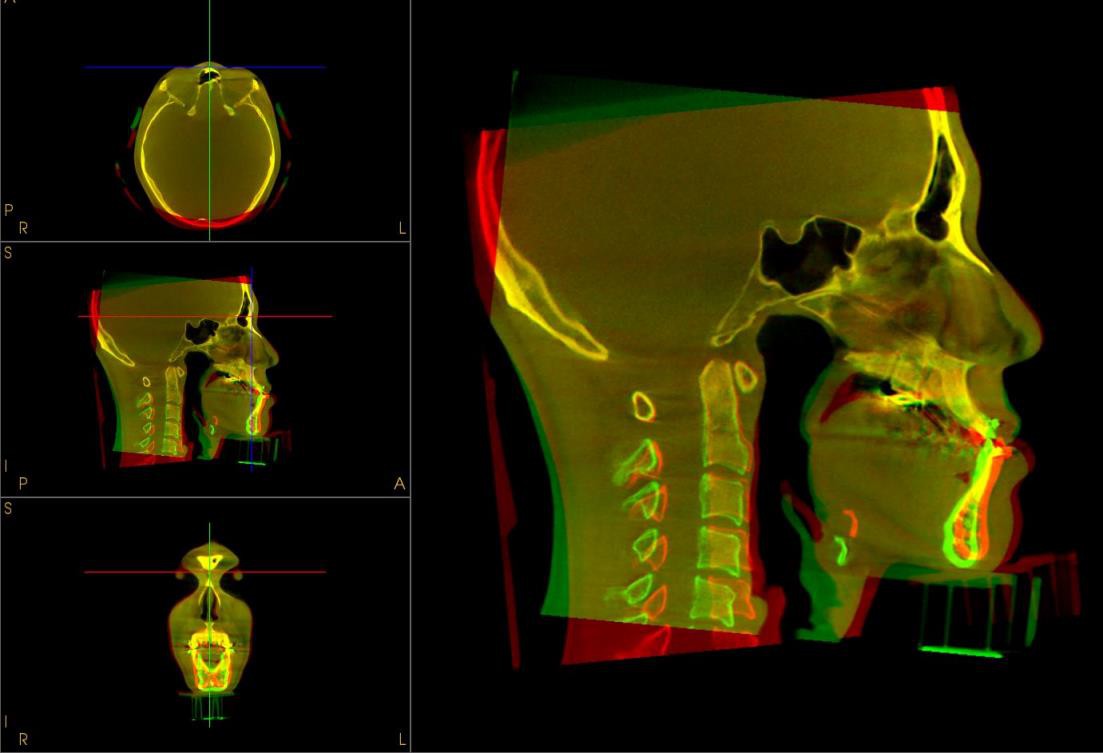
This 15-year-old girl visited our clinic after completing two rounds of orthodontic treatment. The patient wanted to undergo double jaw surgery. Should we wait until her growth is complete to perform the surgery? If so, the misaligned face and body will continue to remain distorted. Even if double jaw surgery is performed after growth, the distorted face and body will continue to be misaligned. It is difficult to correct a distorted facial bone with double jaw surgery because only the front parts of the upper and lower jaws are cut and aligned. The following images show the changes in the misaligned facial and cervical bones after about two months of Invisalign treatment and MCB splint therapy.
As shown in the above illustration, if the misaligned temporal bone is left as it is and only the front part of the lower jaw is cut and aligned, all the cranial bones will continue to move in the direction of distortion, leading to lifelong misalignment. This continuous misalignment will also cause the body's nerves to twist and bend, resulting in a twisted and bent posture. Since the misaligned lower jaw is connected to the facial bones (as shown in the far-right image), the distorted facial bones and body can be corrected using an MCB (mandibular cranial balancing) splint, which is designed to align the center of the lower jaw with the center of the face.
------------------------------------------------------------------------------------------------------------------------------------------
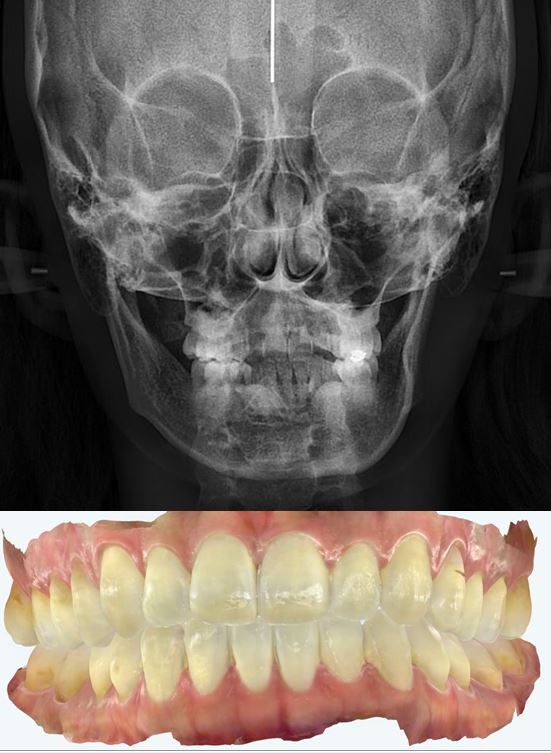
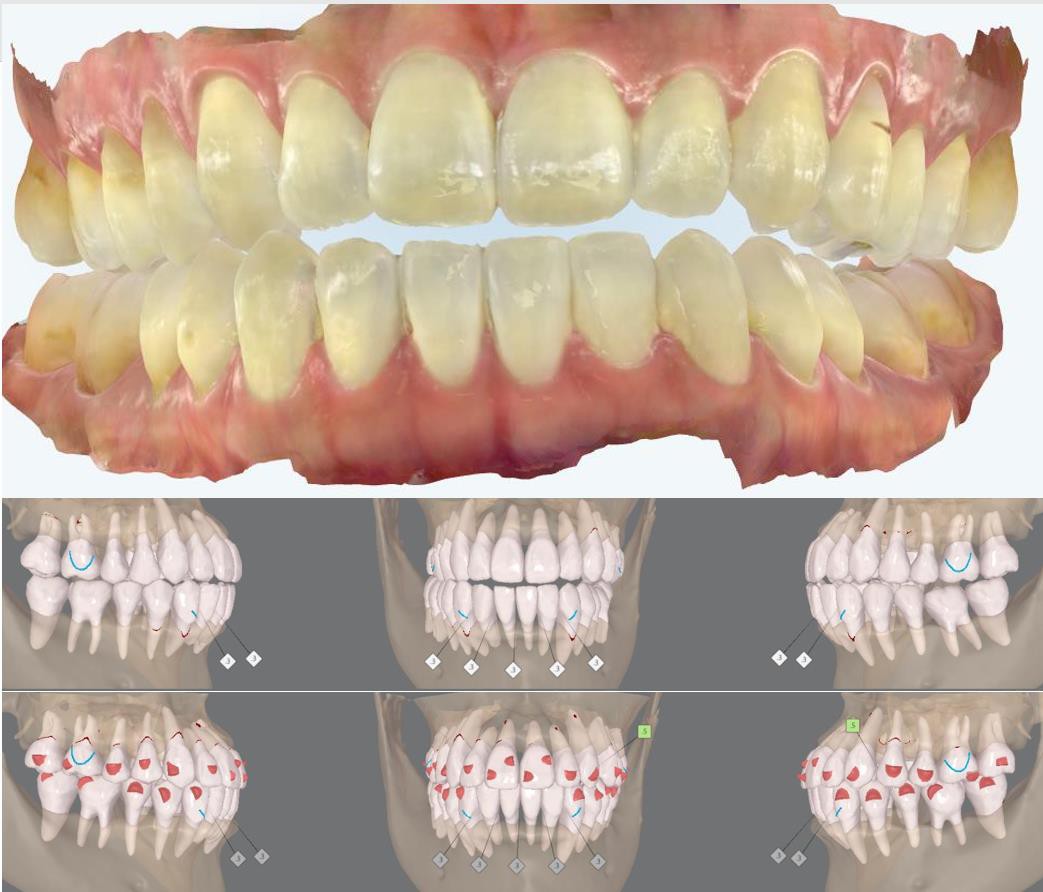
I have already undergone orthodontic treatment, but I am experiencing the following symptoms: My left jaw catches when I open my mouth wide. When I open my mouth wide, my lower jaw moves down in a zigzag pattern. I feel tension in the right jaw muscles. I have allergic rhinitis. My neck muscles easily become stiff. I frequently get pimples along both sides of my neck. I am stressed about facial asymmetry. My left lower back and leg feel tense. My eyes feel strained. My left head, jaw, and neck muscles feel stiff. There is a pulling sensation under my left jaw. Currently, all orthodontic treatments focus on aligning the teeth to a position where they fit well, just arranging the teeth. I have already undergone orthodontic treatment; do I have to live with these symptoms as they are?
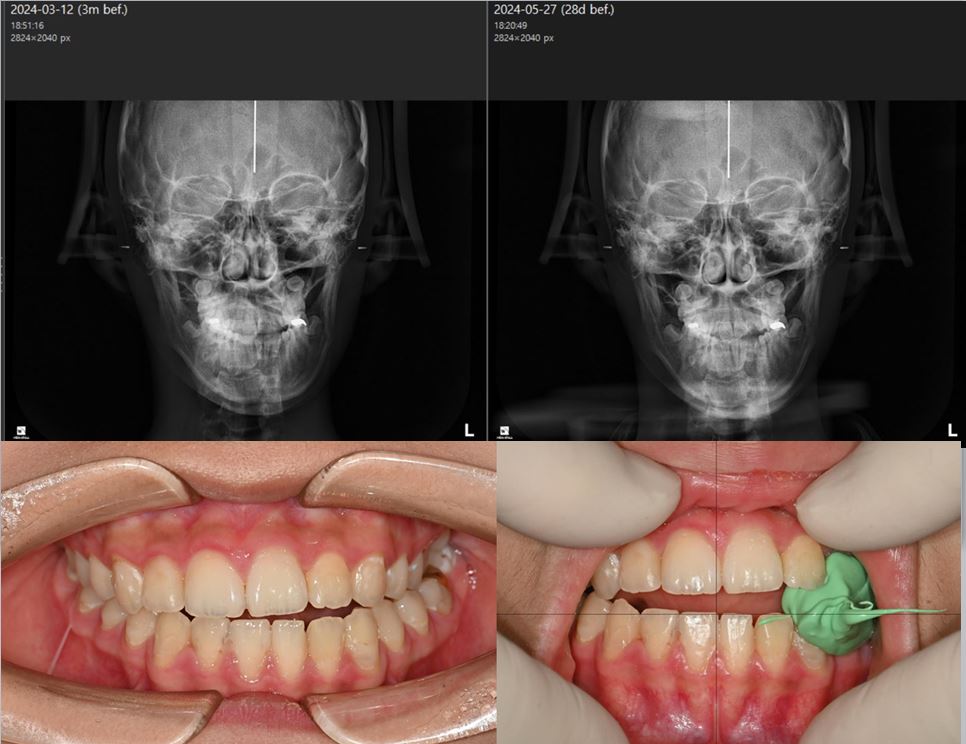
The teeth are currently biting together.
We should not continue treatment in this occlusal state.
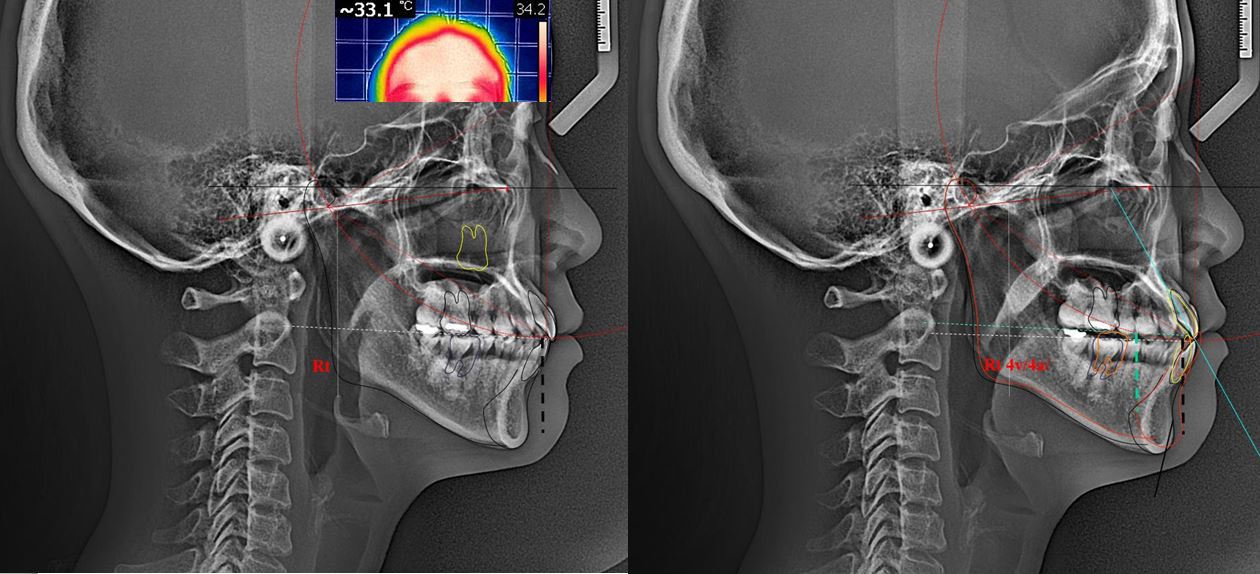
Lateral X-rays show that the chewing force is not being transmitted through the first molars of the maxilla but is instead being directed towards the front teeth.
Infrared facial photographs reveal high temperatures due to poor circulation in the frontal bone.
After aligning the left and right centers of the lower jaw with the center of the face, the occlusal status and lateral X-ray are taken. The maxillary molars must be intruded so that the chewing force is transmitted to the maxillary first molars and distributed through the zygoma.

After 6 months of Invisalign treatment, the symptoms are improving as the lower jaw is shifting to the right. The current orthodontic method, which aligns the teeth in their existing positions, needs to be changed. This is because the lower jaw can be moved without surgery.
------------------------------------------------------------------------------------------------------------------------------------------
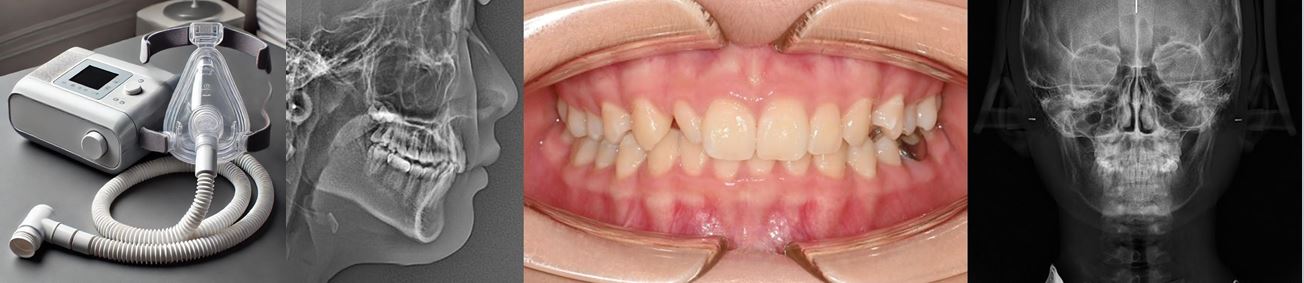
A 13-year-old girl has stopped using her CPAP machine.
If you or a family member has a similar condition, what treatment should be considered first?
Can orthodontics provide a solution?
Or do you think surgical intervention is necessary?
This information is intended for those wondering what treatment might allow someone to live without a CPAP machine for the rest of their life.

We started the treatment by combining the ALF (Alternative Lightwire Functional) device and the twin-block device. Here are images of the device being worn.
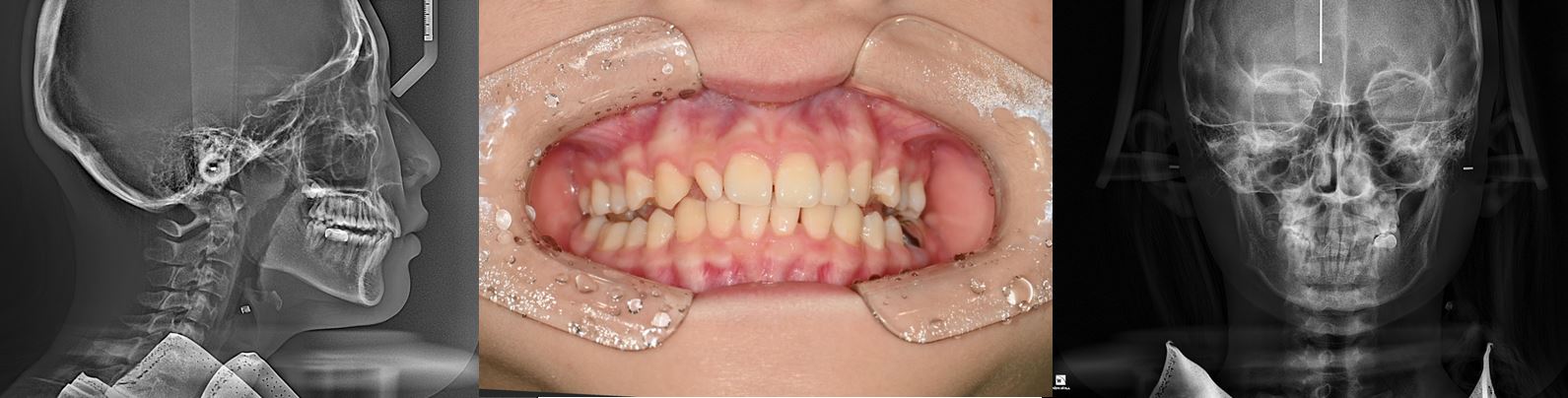
After 5 months:
The twin-block device was made and modified to find the three-dimensional position of the mandible that normalizes cranial bone movement.
During the twin-block treatment, the deep bite was reduced, and asymmetry improved.
However, the PA view showed a reduction in the left nasal space and a tilt in the nasal base.
This tilt was attributed to severe bruxism, which caused resin detachment in the twin-block device.

After 6 months:
The forward movement of the mandible showed changes in the cervical curve.
The nasal tilt became more horizontal than initially.
Additionally, the center of the mandible moved closer to the facial midline.
A sleep study was conducted in this state, and the oxygen saturation improved from 70% to 95%, indicating that the use of the CPAP machine was no longer necessary, giving this student a new lease on life.
In this state, it is better to use Invisalign to correct the asymmetry rather than traditional braces.
------------------------------------------------------------------------------------------------------------------------------------------

The purpose of an aligner chewie is to increase the fit between the teeth and the aligner, ensuring there are no issues with tracking and it is used during the day. However, a kchewie is used for the purpose of TMJ treatment during Invisalign therapy. It is made to align the center of the lower jaw with the left-right and front-back center of the face at a height that allows the occipital bone to move. When worn, it corrects the misaligned facial bones and simultaneously moves the misaligned body in the opposite direction. This device is primarily worn during sleep, allowing natural alignment to occur during sleep, and it enhances the fit of all teeth and the appliance, improving the speed of tooth movement.
------------------------------------------------------------------------------------------------------------------------------------------
Overall, the brain waves show a stable pattern. Delta waves appear to have decreased overall, reducing brain fatigue. Theta power also decreased in the frontal lobe, which is believed to have alleviated the deterioration of the frontal lobe brain function. The increase in alpha waves remains but shows a reduced pattern compared to before. Beta waves are the most normalized than before and show a great improvement in anxiety patterns.
Lee, Jaewon.
M.D., Ph.D. for brain-engineering, Psychiatrist.
Even if you have had surgery on your head, the movement of your skull improves and your brain waves change.
------------------------------------------------------------------------------------------------------------------------------------------
※ Where are the three dimensions of a well positioned mandible?
Even if the lower jaw gets unbalanced by 0.5mm, the whole body including the face get unbalanced and gets worse by time.
These are the consequences that are most likely to occur when the teeth touches the oddly positioned mandible.
Our skull and face that was twisted, oddly positioned and unbalanced will even get worse throughout the time and leads to the increase of tension in the brain’s dura mater and due to the tiny movements of the skull, the brain’s nerves will be disrupted and will eventually cause a problem in the process of the brain sending out messages throughout the body. We can determine these by:
1.If the teeth touches the oddly positioned mandible, we can feel our eyeballs moving a lot faster (can feel the vibration through our finger when we touch the eye). On the other hand, the Temporomandibular joint also known as TMJ starts to move and rotate towards the wrong position, which has a co-relation with the skull and TMJ being unbalanced.
2.There will be a problem in the cycle of blood flow (oxygen). We can determine this by the difference in blood flow of the blood vessel between the supraorbital and supratrochlear artery when our teeth touches the oddly positioned mandible. This blood vessel is located in the skull on top of our eyebrows and it provides blood flow. And if the mandible is twisted and oddly placed, whenever the teeth touches the mandible, it lessens the blood supply of the skull.
3.All of the body parts from top to bottom will slowly fall down which is the key to start twisting and be unbalanced. The front shoulder and the waist will twist in opposite ways of each other and will lead the internal organs to twist as well. If the patient is treated wih an MCB splint, all the muscle of the body parts will no longer fall down and will even help go back up. Therefore the body will be straightened, wrinkles will be lessened and eyes will get bigger. As we can see in the image attached, as long as all the muscles have the movements of going up including the onces in our face, our eyes will get bigger, wrinkles will slowly disappear and as we get old our body posture will still be in good shape making us live a healthy life without pain.

4.The self healing function in our body will be much slower which makes our immune system poor. The proper movement of the skull is really important. Especially in this global pandemic of the coronavirus where we really have to take care of our immune system because we need to rely on them, not only the corovavirus but whatever virus that's bound to happen in the future because at the end, the immune system keeps us safe from all of those.
The movement that goes to the opposite direction above is called the MCB (Mandibular Cranial Balancing) position. If the lower jaw is unbalanced from left to right sides, it makes sphenoid bone unbalanced too. If the lower jaw is unbalanced from front to back, the temporal bone gets unbalanced at the same time. The MCB position is the one and only right position from left to right and front to back, the height of the dental interlocking should be exact for this MCB position for the occipital bone to move normally and properly.
If you press the muscles on the outside of your right thigh with two fingers right now, you can usually feel the muscles sliding down within 1-2 seconds. This indicates that your body is tilting to the right. However, when using the MCB device, the muscles no longer slide down and instead rise back up within a second. In conclusion, MCB splint treatment is necessary to create proper movement in the skull, and if the skull moves normally, you can feel the muscles rising even without the MCB splint device. Therefore, our body posture will be balanced, and uncomfortable symptoms can be prevented.
In the skull, you can see that all the skull bones move in the direction where they do not move upon palpation, and this is correctly arranged in the three-dimensional direction. In this movement, even when the sphenoid bone and maxilla are twisted in the same direction (torsion) or in opposite directions (side-bending), you can feel the three-dimensional movement in the non-distorted direction. All dental treatment should be performed in a position where the three-dimensional position of the lower jaw is not altered by each skull. Through this treatment, not only the dentist himself, but also his family, patients, and everyone on the planet will be happy.


------------------------------------------------------------------------------------------------------------------------------------------
------------------------------------------------------------------------------------------------------------------------------------------
------------------------------------------------------------------------------------------------------------------------------------------
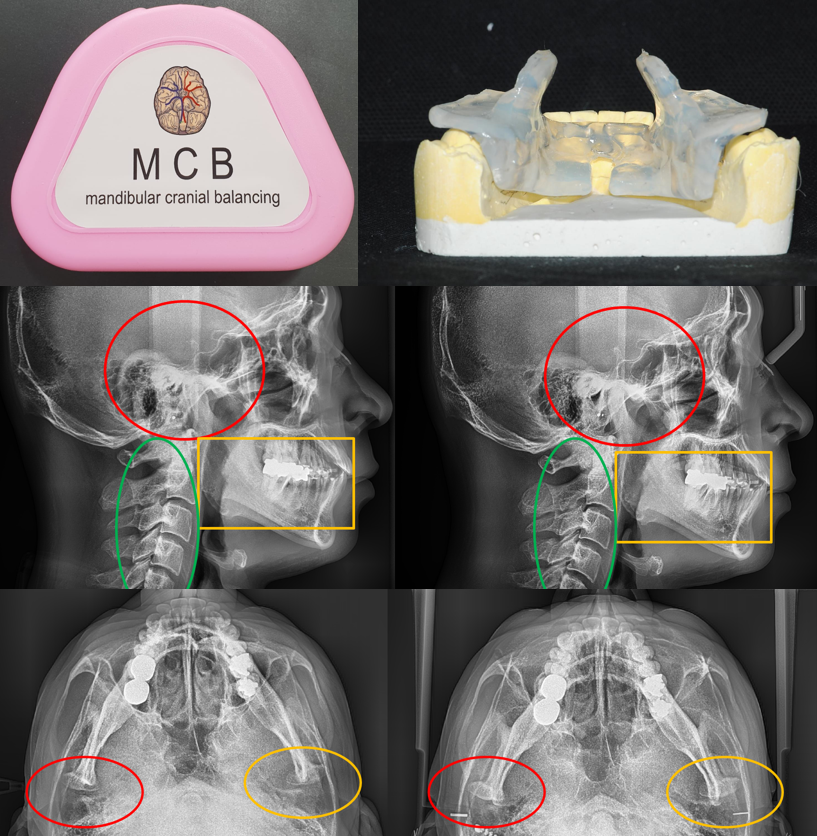
Before, as indicated in the red circle, it looked like there were two condyle. After nine months of using the MCB device, in the image we can clearly see that it looks like one condyle. Also, as indicated in the yellow circle, we can see the difference between the unbalance of each sides of the lower jaw has been more balanced. On the other hand, the image of the cervial which is the green circle has been less crooked.
The shape and texture of the lower jaw’s condyle has changed including the color of it being more brighter. This means the condyle is well positioned in the right place therefore, the texture will become a lot more harder. This is because the weirdly positioned disc had went back to its right position which leads to the increase of blood supply that passes through the disc which eventually adds in bone. As mentioned earlier, the image above is an image of a patient who had made a customized MCB device (patent pending in five countries) after making a dental model and used the MCB device only when sleeping for 9 months.
------------------------------------------------------------------------------------------------------------------------------------------
※ OverBite Treatment.
Modern people often have underdeveloped upper and lower jaws, excluding cases of lantern jaw (where the upper jaw is less developed, and the lower jaw is overdeveloped).
In such cases, modern people have a temporal bone that rotates backward, causing the lower jaw to move backward as well. Even in adults who have finished growing, the upper and lower jaws continue to twist backward as they develop. This is one of the main reasons we develop nasolabial folds and wrinkles as we age.
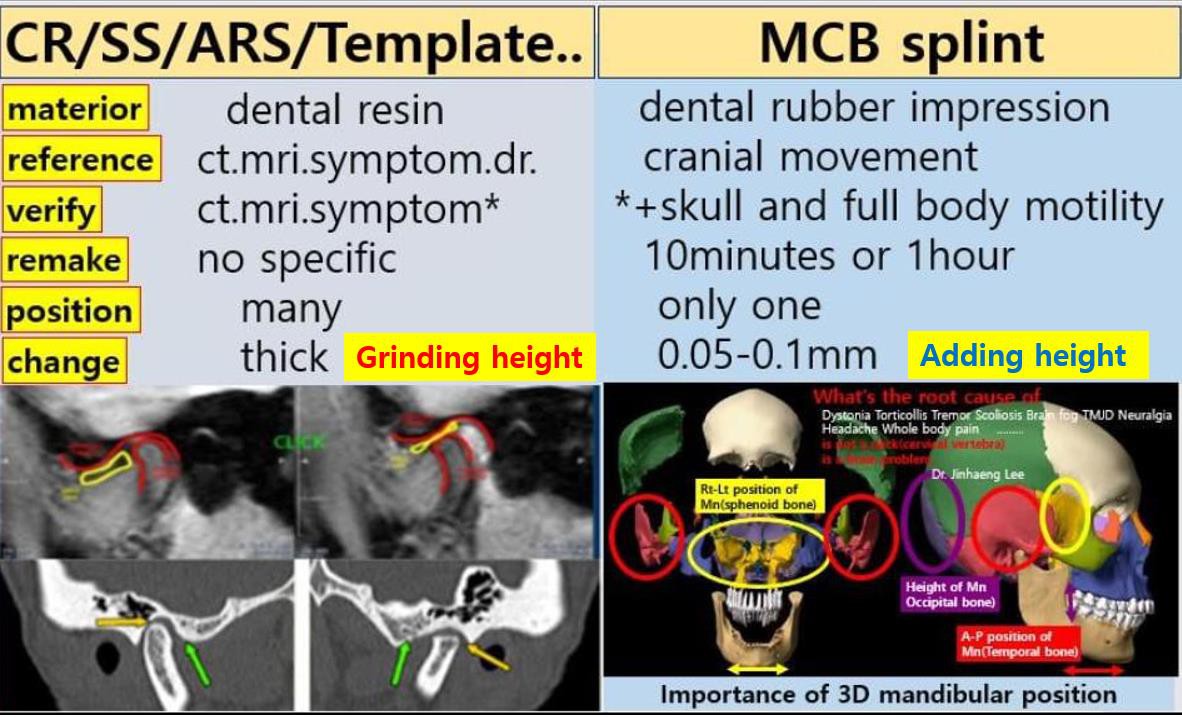
Currently, most dental clinics offer resin-made splint treatment.

This is the oral appearance after resin splint treatment. The lower jaw usually moves backward. The reason this happens is that the splint is made considering only the position of the lower jaw in relation to the temporal bone. When the splint is adjusted in this way, the lower jaw moves to a stable position relative to the temporal bone. However, the new position of the lower jaw is aligned with the twisted temporal bone, while the sphenoid and occipital bones remain twisted. This continues to send signals to our body that they are moving in a distorted manner. Even though we may not consciously recognize these signals, we will live with various uncomfortable symptoms in our bodies.
Adjustment work is done to ensure balanced contact of the resin splint. When the dentist adjusts the resin splint, only the contact areas that interfere with the current movement of the lower jaw are removed to allow free movement and achieve muscle relaxation. However, during splint adjustments, it is crucial to improve the movement of the twisted temporal, sphenoid, and occipital bones to correct the misalignment.
In 1971, Baker published a paper after osteopathic treatment, where he found a slight gap between the second molars of the upper and lower jaws. (Baker EG. Alteration in width of maxillary arch and its relation to sutural movement of cranial bones. J Am Osteopath Assoc 1971; 70(6):559-564). The significance of this paper is that the gap that appeared between the molars after osteopathic treatment suggests that adjusting the three-dimensional position of the molars can improve cranial bone misalignment.
As a result, after trial and error, the MCB splint treatment was developed. This treatment is designed in a position where the sphenoid, temporal, and occipital bones can move well, and the same process is followed during adjustments.
As can be seen in the image below, the further the lower jaw moves back, the more the head moves forward, leading to a straight neck. In a straight neck condition, blood circulation to the brain does not occur as often, and it creates a force that pulls the brainstem downward.
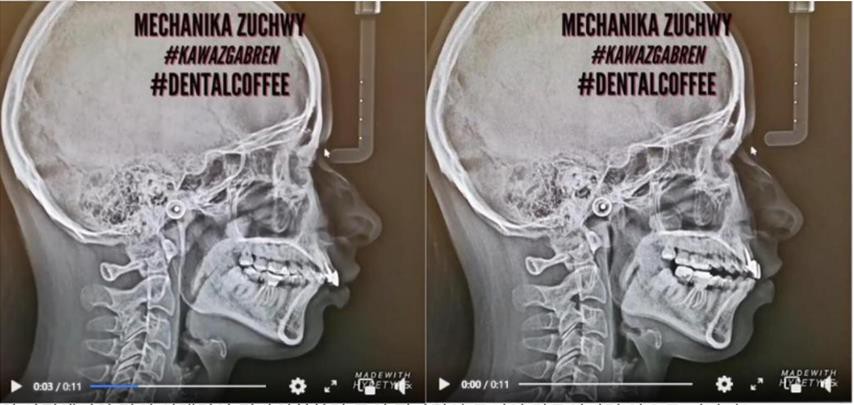
If the lower jaw is positioned forward as shown in the picture above, a normal curve of the neck is created, it does not affect the vagus nerve passing forward, also does not stimulate the sympathetic ganglion and blood circulation is improved. A normal curve like this is necessary for the body to function normally. So grinding the resin splint treatment is a treatment that should be stopped as soon as possible.


If you understand the movement of the skull, you can avoid the treatment of moving the lower jaw back. These days, it is an era of double-jaw surgery, which moves the upper and lower jaw forward in order to secure the hidden jaw.


When occlusal force is transmitted to the first molar, the force applied to the skull is dispersed and absorbed.
The higher the upper molars are raised, the steeper the occlusal plane becomes. At this point, the chewing force is not applied to the first molar but is instead transmitted to the back. When the force is transmitted to the back of the first molar, the force that should be transmitted to the skull and absorbed is concentrated on the condyle of the lower jaw, potentially causing condylar resorption.

Then the condyle will be absorbed.


After tooth extraction and two rounds of orthodontic treatment, the person shown in the image visited the dental clinic due to discomfort from temporomandibular joint disorder.
As shown in the first image, the upper and lower jaws are rotating backwards, but if force is applied to the rear of the first molar, the upper and lower jaws will move further backwards, which causes the skull to receive more twisting force, causing many problems.
However, after the mcb sprint treatment, if the sphenoid bone and the temporal bone of the occipital bone do not rotate backward and move forward well in a balanced state, the upper and lower jaws rotate forward and come out.
In such a state, extraction of the wisdom tooth of the upper jaw can also bring about many facial changes. Since there is no wisdom tooth that was blocking the rearward rotation from the back, it will rotate further backwards.

Two jaw surgery (Jun. 2018) was performed, but facial asymmetry and the upper and lower jaws were retracted (2021.6), which made the jawline worse and the teeth occlusion was not good.
The reason is that when the sphenoid bone and the occipital bone rotate posteriorly as in the picture of 1, the maxilla and mandible recede posteriorly with time. Because only the position of the upper and lower jaw has been treated with surgery and the skull is currently in a misaligned state, the upper and lower jaws retract and move backward as time goes by.
However, when the mcb sprint is attached (Picture 2), the skull moves well and the upper and lower jaws move forward. It is currently 10 months after treatment, and MARPE and Crane were used in the upper jaw to promote forward movement, and the lower jaw was moved forward by mcb sprint (2022.1). This forward movement move more forward when the occipital bone moves forward well.

This image is the result after ten months into treatment.

The mandibular condyle has been moved into a good position and bone is regenerating even without the disc.

After the operation (June 2018), the position of the lower jaw, which was anterior, was moved further back in June 2021 by the rear rotation of the occlusal plane.
Even with double jaw surgery, the jaw changes caused by the misalignment of the skull cannot be
prevented. As such, as time goes by, the skull and upper and lower jaws become misaligned.
If double jaw surgery is performed after normalizing the movement of the skull, the upper and lower jaws will remain unchanged after surgery. So, if you need to have double jaw surgery, it is recommended to use the mcb splint to treat the distortion of the skull before performing the surgery.
With the use of MARPE and the face mask(The Crane), the upper jaw moved to the anterior position, and the lower jaw moved forward due to the change in the position of the temporal bone by using the MCB splint(2022.1).

When the position of the temporal bone is changed while the lower jaw is misaligned, the lower jaw can easily move to the right. If the teeth are aligned by moving the teeth, the face and body become increasingly distorted. In Picture 1, the second cervical vertebra, which was rotated to the right, automatically moves to the center of the face when the lower jaw moves to the right.
The same thing may happen to you. Orthodontic treatment that simply arranges teeth without considering the skull or temporomandibular joint can occur at any time. The following is the state of the patient's skull misalignment. That is, the sphenoid bone and occipital bone have shifted downward to the left, and the occlusal plane of the maxilla has shifted downward to the right. In osteopathic terms, this is called a left sidebend rotation. This indicates a skull misalignment when viewed from the front. There are also distortions on the side and horizontal planes.
If you have an orthodontist who is aware of such cranial distortions, you can trust their orthodontic treatment.
However, most orthodontists perform treatment by using orthodontic screws to raise the right side that has been lowered. If the right side of the maxilla is raised, the tilted occlusal plane may become horizontal. It may seem as though the treatment is successful, but this is because the sphenoid bone is moving well in the wrong direction.
If you undergo this kind of treatment, the skull will become more deformed. Sensitive people may feel discomfort, but most people can go through orthodontic treatment without feeling discomfort. As time goes by, you may start to feel various discomforts and visit multiple hospitals for CT and MRI scans, but the results will come back normal.
However, if you meet an osteopath or dentist who can inform you that your skull is distorted, only then will you be able to understand the root cause. If you only receive orthodontic treatment that focuses on arranging your teeth beautifully, you may live a life filled with pain.
How to treat such a deformity of the skull?

For the sphenoid bone, the lower part of the left side should go up. The occipital bone should also rise on the left side. In the picture on the left compared to CT, you can see the change from before to after treatment.

If you apply force to raise only the lower right side of the maxillary occlusal surface using an orthodontic screw, other bones may become misaligned. When comparing the CT scans after treatment, you can see that the left side has gone down after treatment.
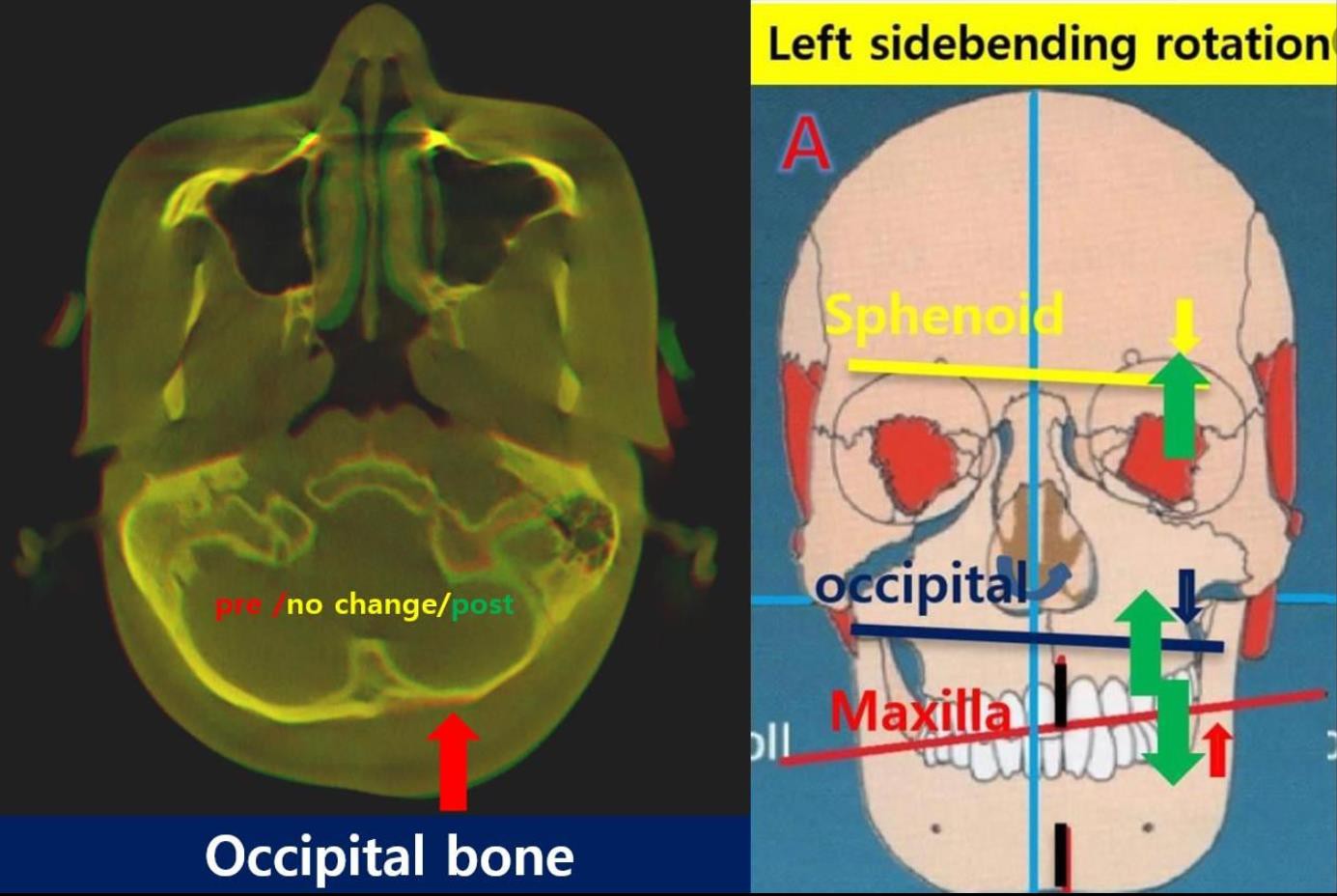
If you look at the CT comparison of the occipital bone before and after treatment, it can be seen that the lower left side has risen up after treatment.
So, are these changes a therapeutic change that can be achieved throughout an artificial osteopathy?
This misalignment is improved by making the three-dimensional position of the lower jaw in a position where the skull moves well. This is a change that happens automatically when you wear the MCB splint. A good left and right position of the lower jaw allows the sphenoid bone to move normally.

A good anteroposterior position of the lower jaw normally moves the temporal bone.
This is because the height of the teeth at this time moves the occipital bone normally
Bilateral balanced Bodily Expansion(Maxilla)
As for the maxilla, the cranial torsion was improved by the use of the mcb splint, so balanced expansion was achieved in both directions with MARPE, resulting in parallel expansion rather than oblique motion, whereas the mandibular teeth were tilted with ALF.

In the maxilla, it was moved forward by traction with The Crane (Face mask) at the same time as the skeletal expansion.

In the mandible, it was moved forward movement by mcb splint at the same time as the dental expansion by ALF.
※ UnderBite Treatment.

There is a severe underbite with a protruding jaw.
Should we proceed with the double jaw surgery that is currently being performed worldwide?
The treatment plan is to normalize the movement of the skull using the MCB splint. MARPE and a face mask will be used for the maxilla, and ALF will be used to expand the dental arch for the mandible, thereby improving the movement of the sphenoid bone and allowing the maxilla to rotate and move forward.
At this time, you can use MARPE to expand the maxilla and simultaneously use a face mask to increase movement.
If skeletal expansion is performed using only MARPE without improving skull movement, asymmetric expansion may occur.
Currently, we are reducing asymmetric expansion by applying MARPE (slow expansion), Invisalign, and the MCB splint simultaneously.
The reason why you, as an adult, need osteopathy or mcb splint when you expand with MARPE!
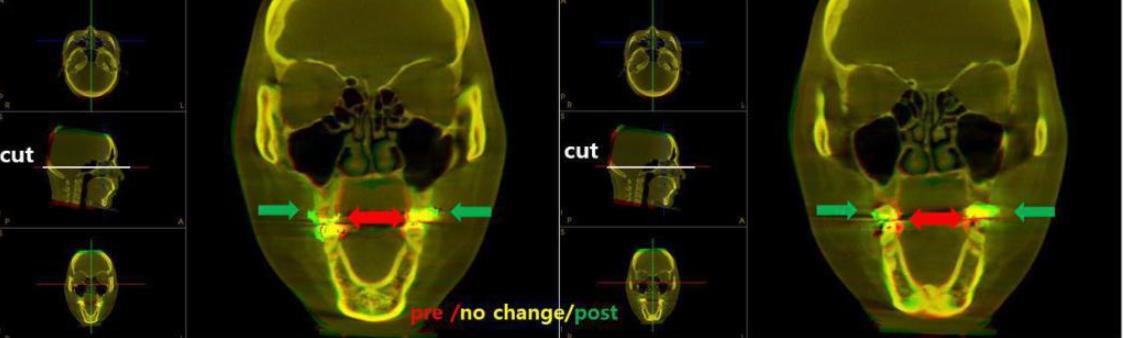
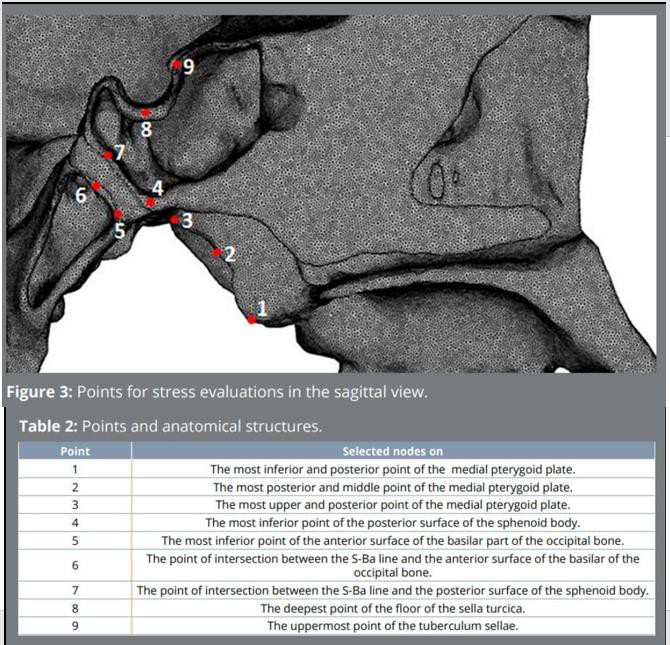
New highlights on effects of rapid palatal expansion on the skull base: a finite element analysis study
Objective:
The objective of this study was to evaluate the effect of
the rapid palatal expansion (RPE) on the pterygoid process (PP),
spheno-occipital synchondrosis (SOS) and sella turcica (ST) in the
skull of a patient with transversal maxillary collapse, and identify
the distribution of mechanical stresses and displacement, by finite element analysis (FEA).
Conclusions:
RPE has a direct effect on PP, SOS and ST in the Class II model skeletal relationship with a transversal maxillary collapse. PP supported a higher tensile stress and displacement.
https://www.scielo.br/j/dpjo/a/fS5NJxYNYT3M7ZJBXQzfmSr/...
During the first treatment, the bone may not be separated because the bone thickness of the maxilla is thick.

So, we plan to use MARPE after confirming bone separation after 2.5 months using a removable extension device. You can see that the bones are separated.
So, we plan to use MARPE after confirming bone separation after 2.5 months using a removable extension device. You can see that the bones are separated.

This is the result 5 months after treatment. Currently, the sphenoid bone is rotating posteriorly, and the maxilla is also rotating posteriorly. Due to the posterior rotation of the temporal bone, the lower jaw has moved to a posterior position.
Is the above change a treatment that can be achieved without surgery?
Why did this change occur?
The upper and lower jaws are part of the skull.
The upper jaw generally aligns with the movement of the sphenoid bone.
If the sphenoid bone does not rotate posteriorly but moves anteriorly as it did after treatment, the upper jaw can also move forward, even in adults.
So why did the lower jaw move backward?
Most people believe that such a change would require surgery to shorten the length of the lower jaw.
This change is related to the rotational movement of the temporal bone.
In the left image, the lower jaw moved forward due to the anterior rotation of the temporal bone.
However, as seen in the right image, the lower jaw moved backward without any change in length because the temporal bone rotated posteriorly.
These changes occur naturally when the skull is corrected and moved with normal movements.
The temporomandibular splint makes this possible.
------------------------------------------------------------------------------------------------------------------------------------------
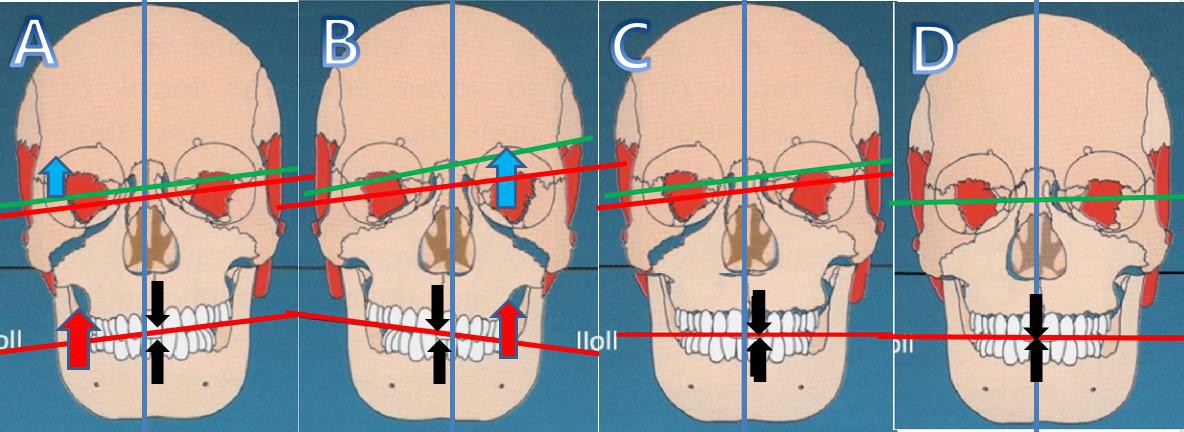
※ Wrong Facial Asymmetry Treatment!!!
Wrong Facial Asymmetry Treatment!!!
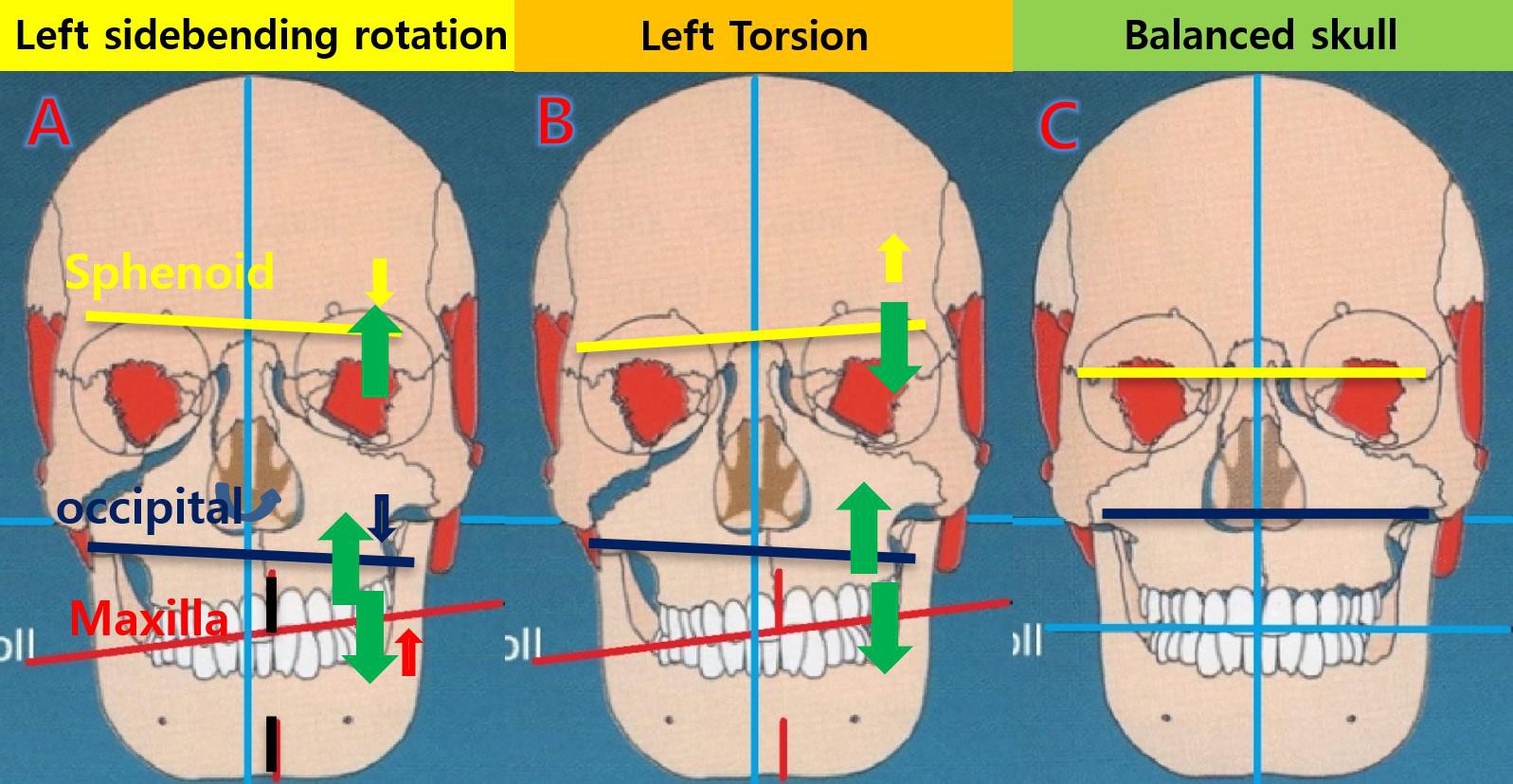
As seen in the image above, in A (left sidebending rotation), both the sphenoid and occipital bones are rotating downward on the left side (ROLL), and the maxilla is inclined upward on the left side.
B (left torsion) is a case where the left side of the sphenoid bone and maxilla is rotating upward, while the left side of the occipital bone is rotating downward.
To date, orthodontic treatment cannot correct the imbalance of the sphenoid, temporal, and occipital bones. When treating the inclination where the left side of the maxilla is elevated, treatment is performed by using an orthodontic screw to raise the lowered right side.
If force is applied to correct the inclination of the occlusal plane without addressing the misaligned bones, the misaligned skull may become more distorted. This is because the bones will twist further in the direction of the existing distortion.
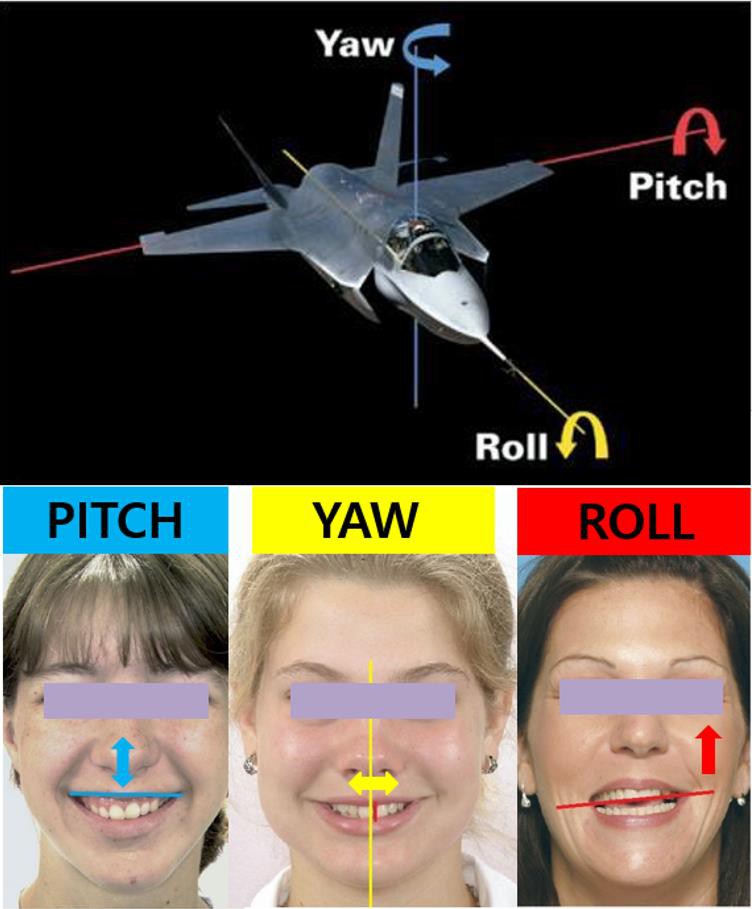
The above treatment method is explained only for the case of ROLL.
Skulls twisted in three dimensions, such as rotation (YAW) and pitch (PITCH), must be treated using the MCB splint or in combination with treatments that increase skull movement.

The above treatment method is only described for the case of ROLL.
Skull that is twisted in 3 dimensions such as rotation (YAW) and pitch (PITCH)
It is treated using MCB splin
※ Any other treatments will make the asymmetry worse!
If there is asymmetry, it moves in the direction it is easy to move. Asymmetric expansion will occur.
Even if you live without treatment, the lower jaw is distorted and you give strength every time your teeth touch, or if you have severe clenching or grinding especially at night, a lot of distorted force will cause the skull to become distorted.

If you apply force while undergoing orthodontic treatment, it will break faster. If the sphenoid-occipital cartilage joint is loosened using MARPE, there is a risk of very much distortion and extension to one side occurs. Easy to move even when maxillary extension is done with ALF (Advanced Lightwire Functional) or MARPE/MSE (Maxillary Skeletal Expander) that expands the upper jaw turns faster in the direction
Why does the left side expand more?

When the sphenoid bone rotates to the left (YAW), the palatine bone also rotates to the left.

Then, on the left, the contact between the maxilla, the sphenoid bone, and the palatine bone is loosened.
Every extension will move the left side more. If you want to treat the left deviation of the sphenoid bone and maxilla, do you need osteopathy?
After MCB splint treatment, the left side distortion disappears and the upper jaw moves to the center of the face will move. This prevents asymmetric expansion and allows for balanced bilateral expansion.
If these distortions are extended without treatment, your face will become more distorted. Everything is affected, including the nerves, circulation, brain function, immunity
Most of the sphenoid bone is rotated to the left, maxilla is also rotated to the left.
Then, can we prevent these distortions and treat the distortion of the skull. You can further increase the movement of the skull bone.
If you receive cranial osteopathy that increases the movement of the skull by an osteopath who can increase the movement of the skull, it may be better.
However, even in the United States, where osteopathic medicine was first started, symptomatic treatment is possible, but there is no osteopath who can increase the movement of 22 skull bones.
Therefore, the upper and lower jaw can not be treated and double jaw surgery is being performed in all countries.
However, double jaw surgery cannot operate on the sphenoid bone, temporal bone, and occipital bone, which is the root cause of a distorted face, but only the front part of the upper and lower jaw. In other words, as time passes after surgery, the face can be slightly distorted, and the distortion of the whole body caused by the cranial bones cannot be recovered.
※ Problems in the current lower jaw surgery (BSSO) treatment.
Problems in the current lower jaw surgery (BSSO) treatment.
The proprioceptors in the human TMJ play an important key role in the identification of mandibular position when the teeth are not occluded. TMJ receptors provide greater afferent activity regarding perceptual awareness of joint position and movement.
In the case of lower jaw surgery (BSSO), it should be performed after correcting the misaligned position of the temporal bone and lower jaw. If a stabilization splint is used to move the lower jaw to a position that matches the misaligned temporal bone (CRO), it is a treatment to move the lower jaw to the misaligned temporal bone.
However, if the three-dimensional position of the lower jaw is placed in the mcb position where the skull moves well, it can be treated while treating the asymmetry by moving the temporal bone. If you do jaw surgery while leaving the misaligned position of the lower jaw and temporal bone intact, you will lose the opportunity to correct the misaligned temporal bone and lower jaw forever.
Then your temporomandibular joint will be in a disorganized state for the rest of your life, sending misaligned proprioception, causing neurologic and neuromuscular disorders, and continuing to make a lot of Substance P.
Then, your overall health will cause a lot of problems.
https://www.hilarispublisher.com/.../recurrence-of-the...
I think the misalignment of the skull is the cause of the misalignment of the upper and lower jaws. So, I think it was the cause of the recurrence of the jaw position after double jaw surgery. //Left roll and posterior pitch recurred after bimaxillary jaw surgery. (5th & 6th picture)


Your problem is a misaligned temporal bone. The lower jaw just followed. If the temporal bone cannot be moved, surgery will be required as it is now.
However, the temporal bone is capable of repositioning.
In the case of lower jaw surgery (BSSO), it should be performed after correcting the misaligned position of the temporal bone and lower jaw. If a stabilization splint is used to move the lower jaw to a position that matches the misaligned temporal bone (CRO), it is a treatment to move the lower jaw to the misaligned temporal bone. However, if the three-dimensional position of the lower jaw is placed in the mcb position where the skull moves well, it can be treated while treating the asymmetry by moving the temporal bone. If you do jaw surgery while leaving the misaligned position of the lower jaw and temporal bone intact, you will lose the opportunity to correct the misaligned temporal bone and lower jaw forever. Then your temporomandibular joint will be in a disorganized state for the rest of your life, sending misaligned proprioception, causing neurologic and neuromuscular disorders, and continuing to make a lot of Substance P. Then, your overall health will cause a lot of problems.

The lower jaw moves to the right.
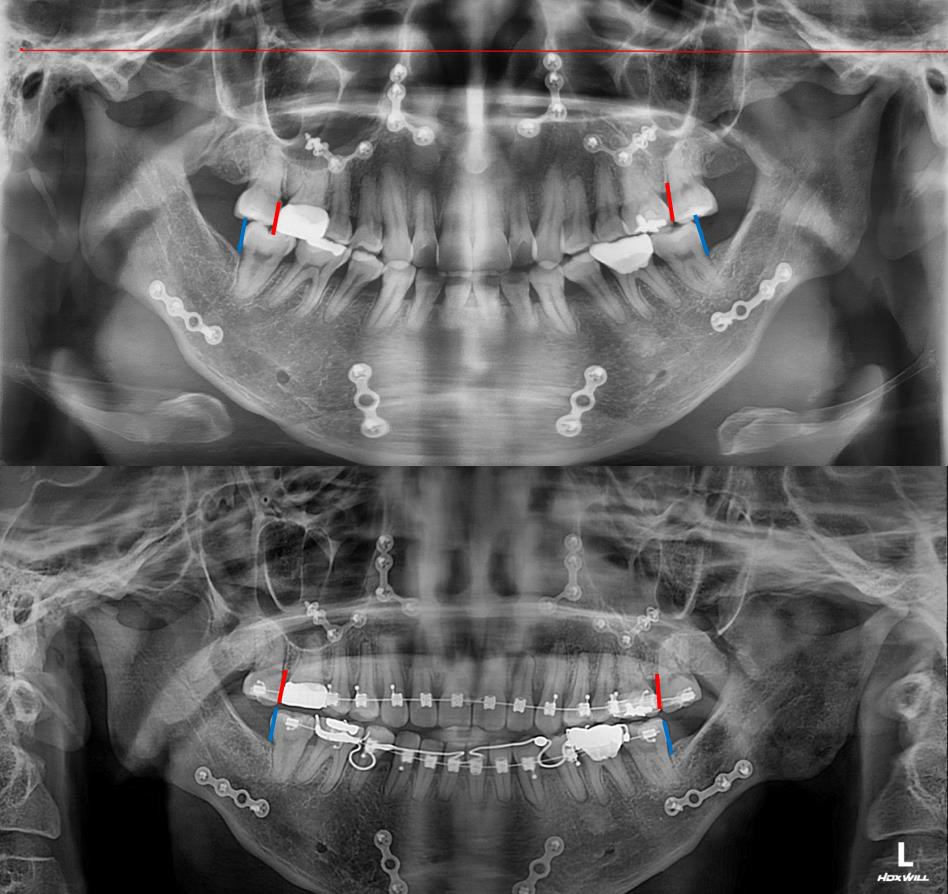
Change of Horizontal Condylar Angle (HCA)It can be seen that from pre (R/31.6 L/32.3) to post (R/32.2 L/25.0), the left yaw of the lower jaw decreased from 32.3 to 25.0 as it moved to the right.

When the lower jaw is in the mcb position, the condyle, the disc, and the temporal bone are in a non-distorted and balanced state. The MOTILITY disappears, and the condyle is regenerated.


Left ROLL after surgery.
After surgery (2018.6), the left occlusal plane was raised upward before MARPE treatment (2021.6). However, after MARPE treatment(2022.1), the left occlusal surface moved downward and leveled. This change is not due to tooth movement, but canting is treated by downward movement of the left side of the upper jaw. In this patient, the left side of the sphenoid bone is raised, and the upper jaw is down on the left side. They moved in opposite directions. These changes are caused by mcb splint and MARPE (The Crane).

Posterior PITCH after surgery.
In June 2021(pre) than after Maxillomandibular Advancement SURGERY (June 2018), both the upper and lower jaw were retracted due to posterior rotation and posterior tilting of the maxillary incisors, but they have positioned anteriorly (2022.1/post) after MARPE (The Crane) and mcb splint treatment. As for the maxilla, the occlusal plane will be flattened by the forward rotation of the maxilla, not the eruption of the teeth, and the lower jaw will also be positioned a little more forward.
※ Steps that change during mcb splint treatment.
The number of splints required for each step is independent of age and is related to the degree of cranial distortion.
1. Anterior-posterior rotation balance of temporal bone.
2. Left and right YAW balance of sphenoid bone.
3. Left and right ROLL balance of sphenoid bone.
4. Anterior-posterior Pitch balance of sphenoid bone.
5. Anterior-posterior balance of the sphenoid bone
6. Left and right YAW balance of maxilla.
7. Left and right ROLL balance of maxilla / The method of raising the lowered part using the orthodontic screw is a treatment that further twists the skull.
8. Anterior-posterior PITCH balance of maxilla
9. Anterior-posterior balance of maxilla.
10. Anterior-posterior balance of premaxilla.
11. Left and right YAW balance of occipital bone.
12. Left and right ROLL balance of occipital bone.
13. Anterior-posterior PITCH balance of occipital bone.
14. A condition in which the sphenoid bone, the temporal bone, and the occipital bone have only normal flexion and extension without mcb splint
15. A condition that does not affect the normal flexion and extension of the sphenoid bone, temporal bone, and occipital bone even if a force is applied in the left and right, front and rear directions of the lower jaw. (me and my wife on Earth)
16. ?
※ Counseling for orthodontic treatment(splint)
Counseling for orthodontic treatment(splint), which has been provided free of charge, is now being converted to video calls for a fee.
Write down all of your uncomfortable symptoms.
Following photos are required to be sent 7 days in advance (prlgresss@gmail.com)
1. All x-ray images(CT/dcm file/21x19FOV)
2. Dental photos
1) Frontal dental view touching with labial frenum exposure
* if you have a splint, add a picture of you wearing it.
2) Side(overjet) view
* if you have a splint, add a picture of you wearing it.
3) Occlusal view of maxilla and mandibular arch
3. Facial Photos
1) Frontal view with showing both ears
2) Side view with showing full ear
4. Full body photos (with light clothes on)
1) Front and rear view with the same position of both feet
2) Side view
5. Bare feet photo
1) Front view
2) Rear view
Please send the above photos 7 days in advance and pay US $200 with Paypal (prlgresss@gmail.com).
Let us know your deposit, and we will start diagnosing it. Diagnosis results are sent by e-mail, and video calls are made about 20 minutes on the scheduled date.
(There is an English interpreter, and the cost varies in other languages.)
The CT image below shows the current state of occlusion. It is necessary to find the three-dimensional position of the lower jaw that normalizes the movement of the skull and perform orthodontic treatment.
※ MCB(mandibular cranial balancing) world seminar.
MCB(mandibular cranial balancing) world seminar.
For orthodontic treatment, splints, and all dental treatments, the 3D position of the lower jaw is only one position. In this position, the movement of the cranial bones is normalized so that the cranial and whole body are gradually shifted correctly, allowing patients to enjoy a healthy life. How is your patient's current lower jaw position? This position must be found by direct palpation of the patient This is an important turning point in any dental treatment.
If you want to participate, please acquire to prlgresss@gmail.com
※ Craniojawtics????
Mandibular Cranial Balancing(MCB) Technique?
MCB technique is a method to make a series of MCB splint.
MCB splint?
a device made in the best position on the lower jaw for the balanced cranial
movement(only one position exists).
Cranial Osteopathy by MCB Splint.
effective for both physiological and non-physiological strain pattern.
Balanced and bilateral amplified movement(cranial and whole body) by MCB splint.
PRM(Primary Respiratory Mechanism) enhancement by MCB splint.
Natural Self-correcting Mechanism of PRM by MCB splint.
Improve circulation by MCB splint.
Improve oxygenation by MCB splint.
Boost immune system by MCB splint .
Neurologic reorganization by MCB splint.
Motor Nerve disorder by MCB splint
(Pyramidal tract./ Extrapyramidal tract).
Strengthen the voluntary muscle.
Body does not collapse any more by MCB splint.
Realine the shoulder and pelvic bone by MCB splint.
TMJ treatment by MCB splint(reorient tmj appratus).
Nonsurgical Facial Asymmetry treatment(balanced face even in the banana-shaped face)
by MCB splint +ALF(Advanced Lightwire Functioals) /MARPE
Doctors who cannot palpate the skull do not know at all whether the patient has yaw and do orthodontic treatment to align only the center of the lower tooth with the center of the upper tooth.
The important thing is to center the upper jaw with the center of the skull, center the lower jaw, and center the teeth. Only the patient himself has to live his life with discomfort. Orthodontists, don't just look at teeth to treat, you need to know and treat the condition of the skull so your patient won't suffer for a lifetime. Orthodontists have to study cranial osteopathy!!
The criterion for developing the upper jaw forward is the position of the lower jaw. In other words, the standard for developing the maxilla forward is to place the lower jaw in a position that does not alter the movement of the temporal bone and place the maxilla in harmony with it.
The same applies to the current MARPE treatment.
I classify orthodontists into two categories.
The first is a doctor who knows the three-dimensional roll/yaw/pitch of the upper jaw (sphenoid bone) before treatment, and studies osteopathic medicine that treats these distortions in the direction of treatment by some dental treatment.
The second doctor is a doctor who does not know the distortion of the maxilla and just treats it. If the lower jaw is in the wrong position and bites and gives strength every time you chew, the patient's skull (brain) will change over time. Patients, you have to study hard to live healthy forever!!
※ Why MCB splint is needed for orthodontic treatment.
1. It protects teeth and jaw joint from clenching or bruxism at bedtime (MCB/L)
2. It stimulates good movement and motility of the skull even at bedtime, because the whole body is relaxed by reducing harmful stimuli so that you can take a deep sleep. (MCB/L)
3. It is a device used at bedtime and during the day and it increases the movement and motility of the skull, enabling rapid treatment of the bodily symptoms.
4. When using MARPE, it increases the mobility of the skull and enables the bilateral expansion of the maxilla. Therefore, asymmetric facial treatment can be performed.
5. When using MARPE, it is easy to move to the front of the maxilla by increasing the mobility of the skull.
6. When using MARPE, it is easy to correct the roll yaw of the maxilla by increasing the mobility of the skull.
7. When two jaw surgery is required, it can be used in conjunction with MARPE/ALF to simplify double jaw surgery by securing a balanced position for non-operative areas such as sphenoid bone, temporal bone, occipital bone, parietal bone, frontal bone, cheekbones, etc.
8. It reduces working and balancing interference by aligning the left and right centers of the upper and lower jaws and teeth.
9. It reduces protrusion interference by aligning the center of the upper and lower jaw and the anteroposterior center of the teeth.
10. By aligning the upper and lower jaw and the left and right centers of the teeth, the occlusal force can be transmitted to the long axis of the teeth in the molar area.
11. Orthodontic treatment is a means of holistic treatment to treat the whole body out of the aesthetic tooth arrangement.
12. Orthodontic treatment can improve brain function.
13. It helps maintain a younger-looking face by reducing facial wrinkles and increasing skin elasticity during orthodontic treatment.
14. It is possible to change the position of the temporal bone and the lower jaw so that the fundamental jaw joint treatment is possible.
15. Orthodontic treatment can treat internal organ problems caused by brain nerve problems due to changes in normal motility of the skull.
16. After the end of orthodontic treatment, the skull can be occluded in the three-dimensional position of the lower jaw that normalizes the skull, so every time the teeth are occluded, the skull bones show good movement.
17. It prolongs one’s lifespan by normalizing the vagus nerve of the person working with the head bent (ex. dentist).
18. During orthodontic treatment, it is possible to prevent the phenomenon of the twist of the sphenoid bone, the upper and lower jaw, and if a twist occurred in the previous orthodontic treatment, it can be restored to the previous one.
19. Orthodontists become TOP DOCTOR because they can treat systemic problems such as dystonia, scoliosis, neuralgia, twisted body posture, allergies, and autonomic nervous system dysfunction.

Her face shape changed from a deformed shape to a small, balanced egg-like shape, the height of her left and right eyes also changed, and the temperature of her head and eyes changed to normal red color. This means that blood circulation has improved.
This difference changed even though she lived in the province and her MCB treatments were 20% of her recommended treatments due to coronavirus.
Remenber!!! The face can be twisted(MARPE) or it can be turned back by MARPE and MCB splint.
※ The way humans live healthily is through the bones of the skull to improve movement. Isn't this the Bulloch(herb of eternal youth) that King Jinshi(Qin Shi Huang) looking for?
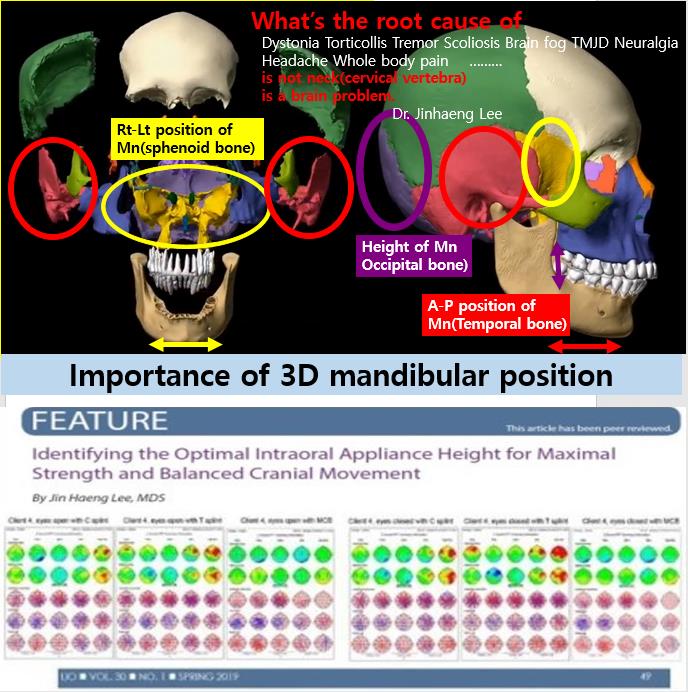
What’s the root cause of
Dystonia Torticollis Tremor Scoliosis Brain fog TMJD Neuralgia
Tic Tourette Neurological disorder Headache Whole body pain……
is not a neck(cervical vertebra)
It's just a branch of one dura mater.
is a brain problem.
The MCB splint improves the movement of the skull, allowing bilateral and balanced movements of both sides. This will relieve tension in the dura mater and can heal problems with nerves in the brain.
When your skull is moving in a balanced way, you can feel the body temperature dropping in the upper part of your head with the back of your hand. This is because the blood circulation in the skull is improved. It promotes the supraorbital artery and supratrochlear artery, and you can feel a stronger, more powerful beat than before.
When the MCB splint is created in a three-dimensional position where the skull movement improves, the twisted skull begins to move in the non-twisted direction, turning into a movement that only expands and contracts. If the lower jaw is twisted to the left, the entire temporal bone moves to the right (and vice versa)), if the lower jaw is protruded, the temporal bone moves backward, and if the lower jaw is moved backward, the temporal bone moves forward. . At the same time, the shoulder, pelvis, spine and internal organs also move in a non-twisted direction.
The first level of MCB splint treatment is that after the device's treatment time (10 minutes), the skull no longer expands and contracts and the skull becomes a little less distorted than before. In this case, when the device is worn, it moves better than when the device is not worn. However, because the distorted skull doesn't move to a good position, we have to build a new device.
The second level of MCB splint treatment is that the movement of the occipital bone shows better movement when the device is worn after the treatment time (10 minutes) has passed. However, in the occipital bone, twisting movements and good movements are repeated.
In MCB splint treatment, the third level is that when the device is worn after the treatment time (10 minutes) has passed, the movement of the occipital bone is no longer distorted, and only good movements appear.
In MCB splint treatment, the fourth level of MCB splint treatment, the treatment time of the device lasts 1 hour.
In MCB splint treatment, the ?th level shows only dilation and contraction, unlike previous movements of the sphenoid temporal bone occipital bone when the device is worn after the treatment time (1 hour) of the device has passed.
I feel that MCB treatment is a necessary treatment not only for people with diseases but also for those who think they are healthy.
https://www.facebook.com/jinhaeng.lee.125/
https://www.instagram.com/jinhaengmcb/
https://twitter.com/jinhaengmcb
https://www.tumblr.com/settings/blog/ljinhaengmcb
Most people's faces are asymmetrical. If there is asymmetry, the movement of the skull bone is distorted. If the position of the lower jaw is misaligned and a force is applied every time it touches, the asymmetry will gradually worsen as time goes on, and at the same time, the body will also be distorted. During orthodontic treatment, this misalignment is more likely to be misaligned. During orthodontic treatment, if you do not know the deviation of the PITCH YAW ROLL of the maxilla and do not treat it in the direction of improvement, it will move better in the wrong direction so that it may be misaligned during treatment. So orthodontists should study osteopathy. MCB SPLINT SEMINAR helps orthodontists treat these problems a lot.
https://docplayer.net/11113860-Pitch-roll-and-yaw-describing-the-spatial-orientation-of-dentofacial-traits.html #mcbsplint
※ Facial bone classification.
Facial bone classification.
Anyone who practices osteopathy develops the sense of the fingers. When you do osteopathy, you can get various information through the senses of your fingers on the body part. In the case of the skull, you can see what the major distortions of the face are currently and how much change is caused by any treatment. This will change depending on the force applied during ALF, MARPE or orthodontic treatment. This information is important biometric information that cannot be obtained through CT or MRI.
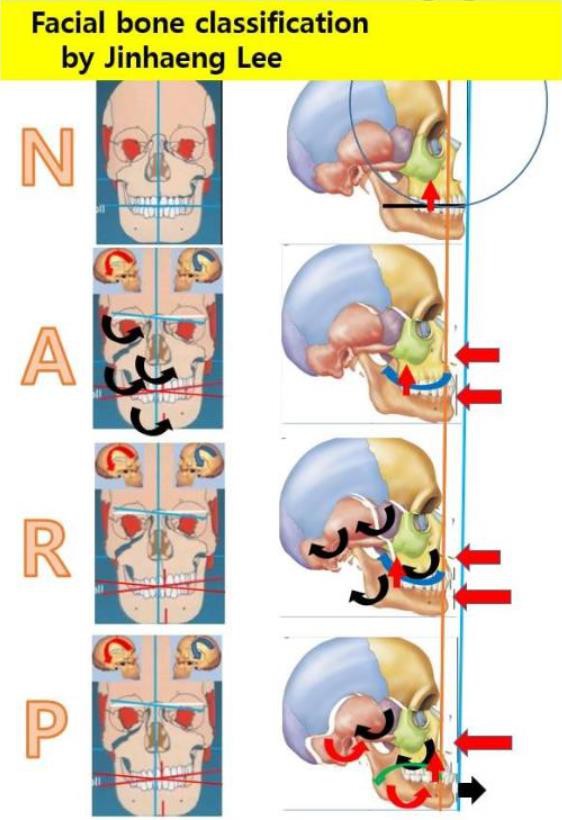
This is the classification I think based on the distortion of the facial bones.
N (Normal type) Everything is in a normal state.
A(Asymmetric type) Mainly, the face becomes asymmetric. The cause is the twisting of the sphenoid temporal bone, which causes the maxilla and mandible to twist.
R(Retraction type/ Angle C2) The upper jaw rotates backward by the posterior rotation of the sphenoid bone, and the mandible rotates more backward by the posterior rotation of the temporal bone. The change of the occlusal plane also changes steeply.
A and R are similar to each other, but are determined primarily by the direction of twisting of the sphenoid and temporal bones.
P(Prognathic type/ Angle C3) The maxillary is rotated backward by the posterior rotation of the sphenoid bone, and the mandible is moved forward by the anterior rotation of the temporal bone. The occlusal plane turns flat.
As soon as I put on the MCB splint made in the position where the movement of the sphenoid temporal bone occipital bone improves, I can feel the movement in the opposite direction twisted by the palpation of the finger. So, if you put on the MCB splint and apply force in the opposite direction, the movement increases and the distortion gradually decreases. This change occurs in the whole body, and similarly, when exercise or force is applied in the direction of improvement, the body no longer twists in the twisting direction.
#mcbsplint
How to treat maxillary canting?
Should the lowered area be treated with an orthodontic screw to lift it up? The tilt of the maxilla is caused by the twisting of the sphenoid bone. In other words, the side where the sphenoid bone descends also descends the maxilla (A). If you come down at the same time like this, you can put the lower side up. However, even if a lot of force is applied to the lowered part, the sphenoid bone does not move and the teeth move mainly. This is because the sphenoid bone moves well in the twisting direction but does not move in the opposite direction.
However, contrary to the inclination of the maxilla, the sphenoid bone may be distorted (B). In this case, if an upward force is applied to the lowered part, the sphenoid bone moves well in the wrong direction, so it moves well. In other words, the sphenoid bone is played even more. The occlusal slope of the maxilla has been treated, but the sphenoid bone is further twisted. In other words, if you do not know the distortion of the sphenoid bone and treat the maxillary inclination, the skull may become more twisted.
For maxillary occlusal canting treatment, while using MARPE to increase the movement of the skull, use the MCB splint at the same time to determine the distorted state of the sphenoid bone, and then treat the distortion of the sphenoid bone. You have to make the cranial movement better.
So, orthodontists must study osteopathy for their patients and themselves.
For maxillary occlusal canting treatment, while using MARPE to increase the movement of the skull, use the MCB splint at the same time to determine the distorted state of the sphenoid bone, and then treat the distortion of the sphenoid bone.
The treatment mechanisms of A and B are treated by completely different treatment mechanisms.
In case A, the sphenoid bone moves in the same direction as the maxilla. In other words, the inclination of the maxillary jaw is treated only when the sphenoid bone moves. If the sphenoid bone does not move, only the teeth will move.
However, in the case of B, the cause of the distortion is completely different from that of A. In other words, it does not follow the motion of the sphenoid bone, but moves in the opposite direction to be treated. This movement can be felt by finger palpation when wearing the MCB splint, the sphenoid bone and the maxilla move in the same direction in A, but in the opposite direction in B. In other words, this movement is possible only when the movement of the skull is increased by wearing the MCB splint.
Even if the teeth are level, the skull bone does not move normally (C).
Even if the teeth fit well, the movement of the skull does not improve (C).
The movement of the temporal and occipital bones as well as the sphenoid bone should be improved.
Therefore, orthodontists should study osteopathy. This is because the force exerted by the teeth affects the skull.
If you treat the occlusal slope of the maxilla without knowing the condition of the sphenoid bone, you may live with many problems after corrective treatment.
※ Does your splint move your skull and whole body?

Does your splint move your skull and whole body?
What is the root cause of the jaw joint problem?
That"s because the temporal bone, disc, lower jaw is distorted.
In order to improve the jaw joint, the temporal bone and disc should move in a good direction when wearing a splint.
The temporal bone moves downward on the right side, both sides move to the left, and backwards. This movement causes the associated bones to move in the same direction.
For example, the pelvic bone usually has a lower left side when lying down, but if the temporal bone is rotated to the right by wearing a splint, not only the lower jaw is moved to the right, but the right side, where the pelvic bone is also high, can be palpated to lower.
If it doesn't move, that splint won't cure you!
Then is it possible to move only the temporal bone?
In order for the temporal bone to move, all the bones around it must move at the same time in order to move the temporal bone.
So is this possible?
It is possible by making a splint after accurately finding the 3D position of the lower jaw.
However, to make this splint, it's only possible for someone who can palpate the movement of the skull.
If you wear the splint made in this way, you can feel the movement of not only the skull but also the twisted whole body with the palpation of the fingers.
In other words, you can correct the twist body as well as the twisted head bone and these things are caused by changes in the nerves. #강남턱치과
※ My observations on scoliosis and Kyphosis.
My observations on scoliosis and Kyphosis.
I always examine the patient while lying down to make a mcb splint.
Until now, the deviation of patients who visited the hospital has always been the same pattern.
The right shoulder is rotating backward, and the left pelvis is rotating backwards.
In this movement, when the mcb splint is installed, the shoulder that was narrowed forward is stretched backward, and the right shoulder that moved backward moves forward.
And the left pelvis, which was moving backwards, begins to move forward.
At the same time, the spine moves straight as all the muscles move upwards instead of downwards.
These movements are consistent with the direction of deflection in scoliosis.
The following x-ray is of a patient who was treated for discomfort in the temporomandibular joint, who underwent short-term mcb splint treatment.
https://www.polyu.edu.hk/.../adolescent.../what-is-ais/
https://www.nature.com/articles/s41598-021-86436-3#Fig1
https://www.hopkinsmedicine.org/.../condition.../kyphosis....
https://www.sciencedirect.com/.../pii/S2395921516300617
https://www.mdpi.com/2076-2615/11/10/2808...



This is what it looks like after having 10 sessions (100minutes) of an MCB splint treatment. The patient does not want any further treatments because the patient does not feel any uncomfortable symptoms. There was a change in the position of the occipital and temporal bone just because the kyphosis in the thoracic spine’s was lessened.(Surgery Patient)



※ What is autonomic dysfunction?
What is autonomic dysfunction?
Autonomic dysfunction develops when the nerves of the ANS are damaged. This condition is called autonomic neuropathy or dysautonomia. Autonomic dysfunction can range from mild to life-threatening. It can affect part of the ANS or the entire ANS. Sometimes the conditions that cause problems are temporary and reversible. Others are chronic, or long-term, and may continue to worsen over time.
HRV = ANS & Stress
How is autonomic dysfunction treated?
*TMJ splint((mcb splint(When the mcb splint is installed, the HRV changes immediately))
*elevating the head of your bed
*drinking enough fluids
*adding salt to your diet
*wearing compression stockings to prevent blood pooling in your legs
*changing positions slowly
*taking medications like midodrine
Nerve damage is difficult to cure. Physical therapy, walking aids, feeding tubes, and other methods may be necessary to help treat more severe nerve involvement.
https://www.healthline.com/health/autonomic-dysfunction
https://elitehrv.com/what-is-heart-ra
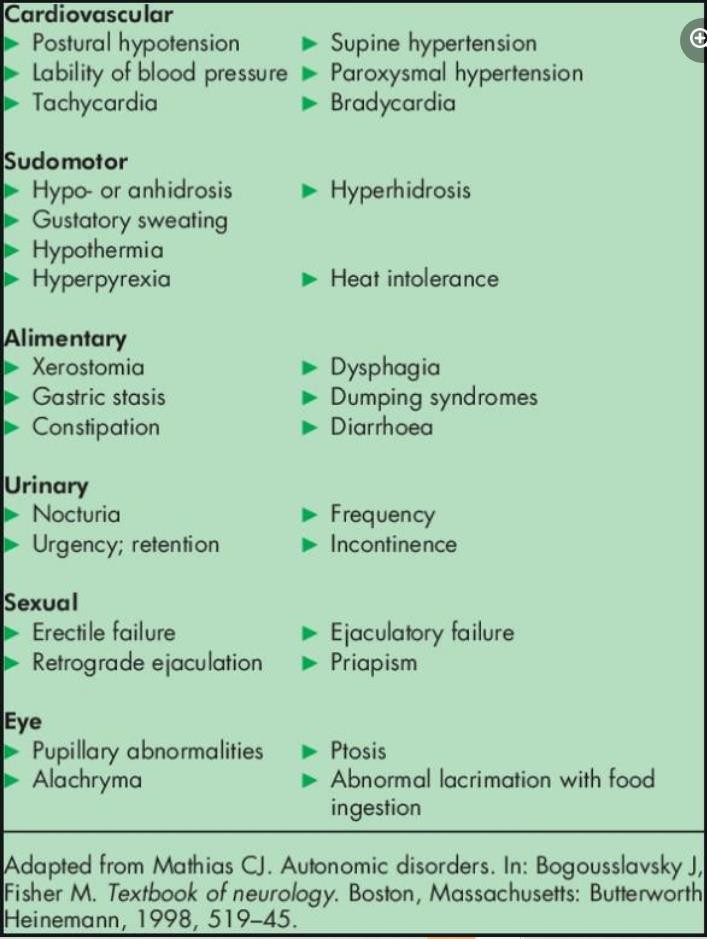
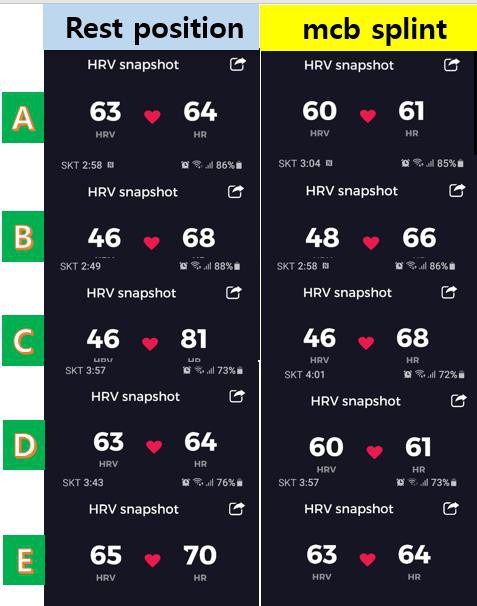


※ An unstable jaw position cannot be stabilized with a splint.
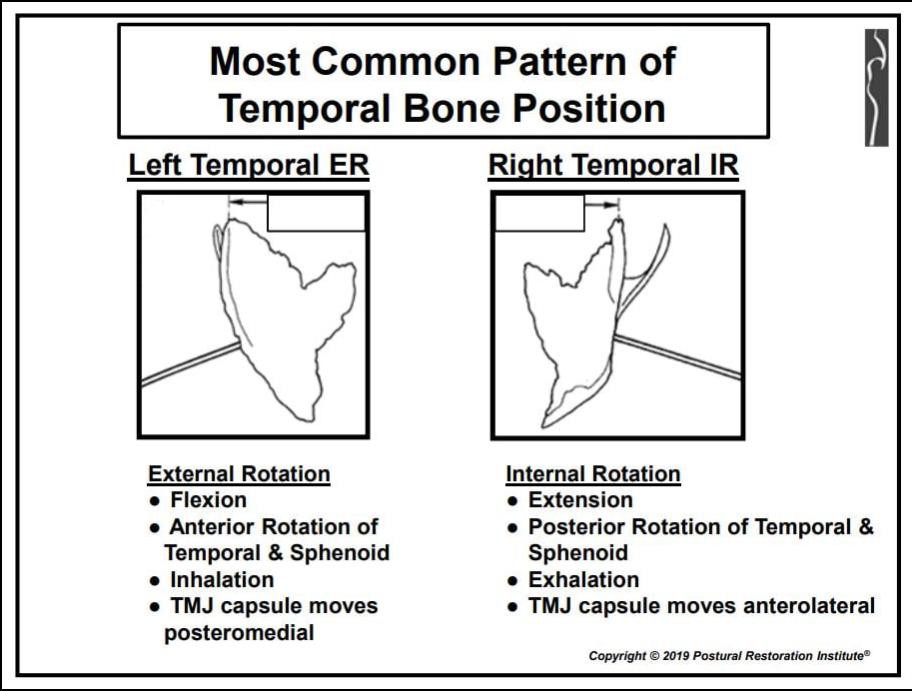

It has been corrected in the distorted direction of the lower jaw. I corrected the position of the lower jaw by facilitating the three-dimensional position of the condyle of the mandible and the temporal bone. Anyone with sensitive finger palpation can do this.

Journal AOA/vol. '78, June 1974
Dr. Magoun is a trustee in the Sutherland Cranial Teaching Foundation,
Inc., Meridian, Idaho.
Mandibular Asymmetry.
With external rotation of the temporal bones, the temporomandibular fossae move somewhat posteromedially, causing a bilateral backward shift of the lower jaw, which may
result in overbiting. Conversely, internal rotation of both temporal bones moves the fossae anterolaterally, which tends to cause protrusion of the mandible
If one temporal bone is rotated internally and the other externally,
which is the common slight deviation, a lateral shift of the symphysis menti to the side of the posterior temporomandibular fossa will occur and will be evidenced by midincisal malalignment. For such a condition, the realignment of cranial bones would seem simpler and more logical than attempts to move the teeth.
False premise.
A possible shift in the relative positions of the two temporomandibular fossae is an important pathogenic factor which has been largely overlooked by the dental profession.
No end of arguments have arisen concerning the mechanics and functioning of the TMJ articulation. Its anatomy has been explored in the minutest detail, but many well-meant conclusions have been based on the false premise that the two articulations are in a relative position of complete immobility.
***An unstable jaw position cannot be stabilized with a splint.
Do you still believe that it will be stabilized after a few months of splint treatment???
This is because the temporal bone continues to move.
However, if the distortion of the skull improves, the movement of the temporal bone can be stopped.
"popping jaw"
The disturbing phenomenon of a "popping jaw" has been attributed to slipping of the articular condyle over the posterior edge of the cartilaginous disk and to its forward movement to hit the articular eminence. Regardless of the cause, normalizing the structure of the whole area is satisfactory therapy in most cases. Proper positioning of the temporal bone is paramount.
MCB splint instantly moves the temporal bone, sphenoid bone, occipital bone, and all skull bones and whole body.
#mcbsplint
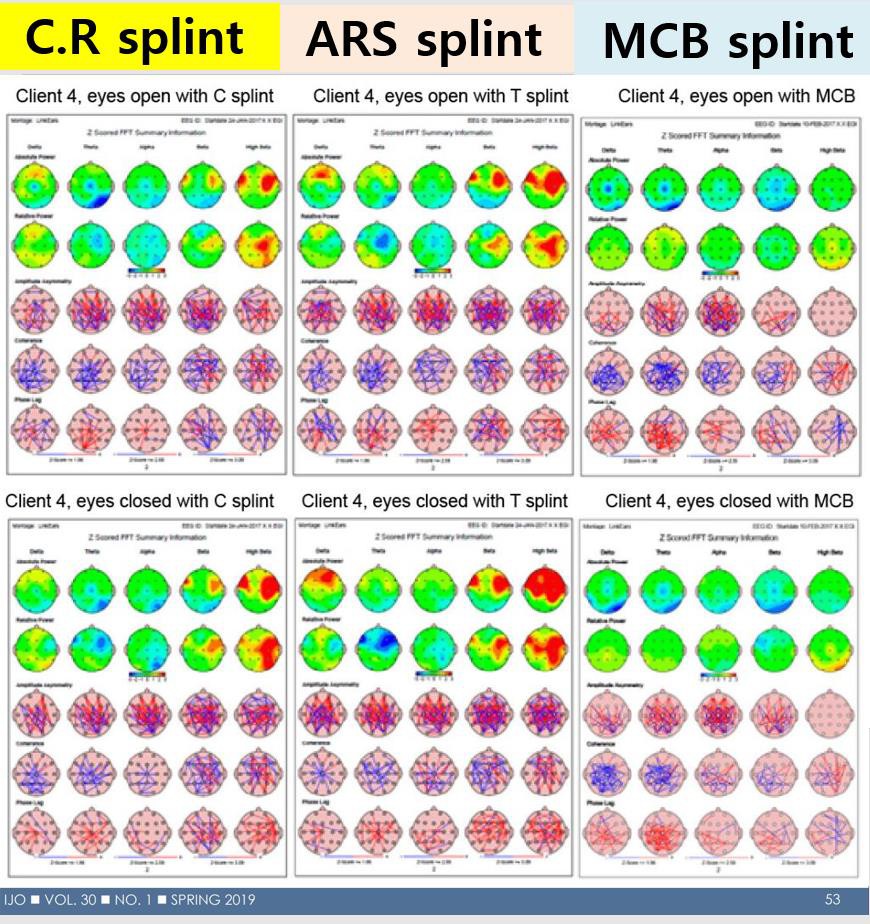


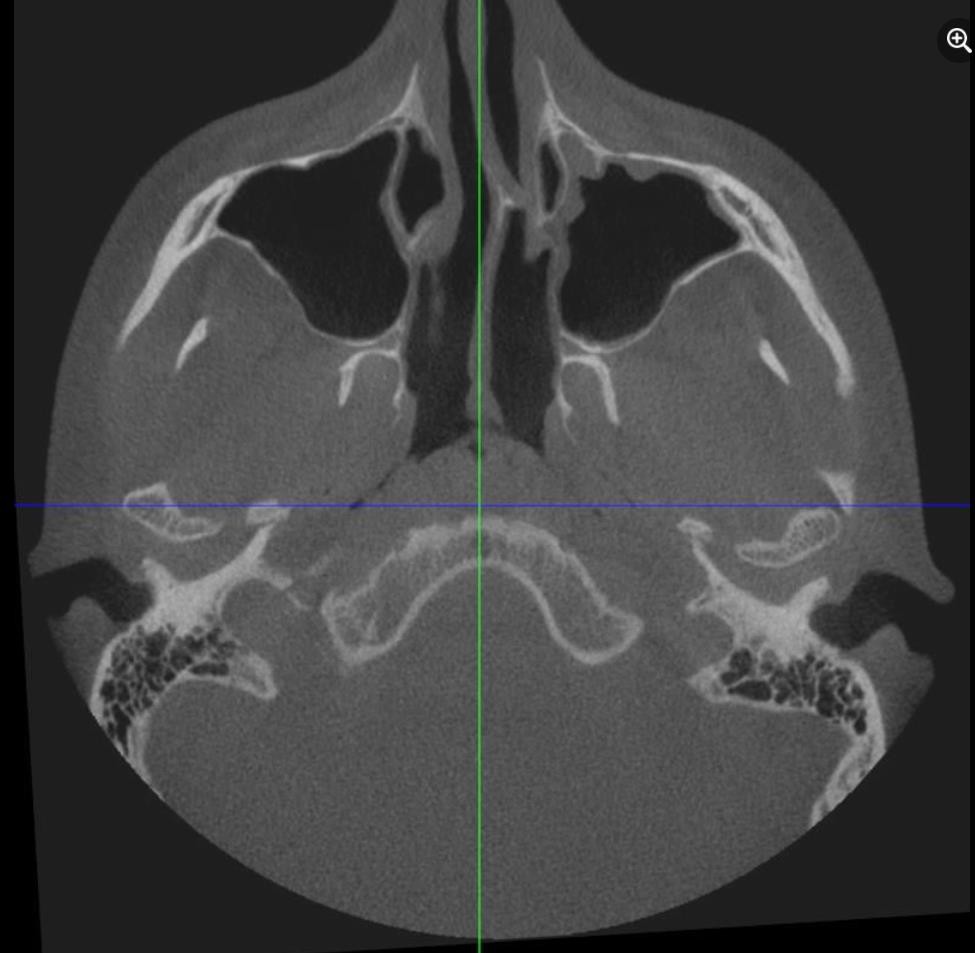
Do you think that the position changed after several months of splint treatment correctly aligns the distortion of the skull and the whole body?
Perhaps after treatment, the skull and the whole body will be more distorted, and the strength of all muscles will be weakened. Your splint does not change the position of the misaligned temporal bone, and the lower jaw is further twisted in a misaligned state. This position is unstable and will change again. After stabilizing splint treatment, the lower jaw and upper jaw are rotated more clockwise, so that the anterior open bite appears and the lower jaw is more left twisted. This is because the left temporal bone is externally rotated. If surgery and orthodontic treatment are performed in this state, the distorted temporal bone will be slightly distorted as time goes by and the body will continue to be distorted. Treatment of intrusion of the maxillary molars to treat anterior open bite accelerates the clockwise rotation of the upper and lower jaws. As a result, when a steep occlusal plane is taken and applied to the molars, the occlusal force is concentrated on the condyle rather than distributed throughout the skull. After the treatment, the anterior open bite seems to have been cured, but the lower jaw has moved more rearward, and the occlusal height that supports the lower jaw is lowered, which further distorts the occipital bone. The first goal of all orthodontic treatments is to make the occlusion of the lower jaw in a position where the three-dimensional position of the lower jaw does not distort the skull. In this way, orthopedic stability can be achieved. Orthodontic treatment should be carried out in consideration of the patient's whole body distortion. If there is MOTILITY in the temporomandibular joint when any splint is worn in the oral cavity, the splint is in the wrong state. #mcbsplint
http://www.thecranencrp.com/
※ The reason my face keeps changing
The reason my face keeps changing
Most people have asymmetry in their skulls. If the lower jaw is in a distorted position, the asymmetry becomes more and more distorted as time passes without treatment.
This is because the twisted lower jaw gives strength to the skull. In other words, even without treatment, the bones of the skull deteriorate over time.
The reasons are as follows:
If the left and right positions of the lower jaw are twisted, the sphenoid bone that has already been twisted is further twisted.
If the anteroposterior position of the lower jaw is misaligned, the temporal bone is twisted further.
If the height of the lower jaw is not correct, the twisted occipital bone is further twisted.
When the dentist moves or makes changes to the teeth for treatment, it starts to twist faster than the natural speed. Particularly with MARPE (miniscrew-assisted rapid palatal expansion), all parts of the skull bone move better and begin to twist faster. Even with ALF treatment, it goes wrong.
The way to prevent twisting is to improve the movement of the skull by performing osteopathy. However, if the position of the lower jaw is in a position that twists the skull, it cannot be prevented from twisting. That's because every time a tooth touches, a twisting force is applied to the skull.
In this case, the MCB splint, which places the lower jaw in a three-dimensional position that normalizes the movement of the skull, prevents twisting and induces normal movement, so that the skull and the whole body are properly aligned by the self-healing mechanism. In other words, when performing the orthodontic treatment, it is necessary to always consider the three-dimensional position of the lower jaw. That is why orthodontists should study osteopathy.
Jose Ortega, one more question, but since the maxilla is articulated with other bones that belong to the skull, the expansion of this will not bring greater torsion in the adjacent bones? Or would it be necessary to perform a previous maxillary surgical expansion to possibly avoid any possible torsion?
·Reply·
Jinhaeng Lee MARPE should be used to expand the maxilla to significantly increase overall skull motility. However, the overall mobility does not increase, resulting in distortion and an increase in asymmetry. However, if you wear an MCB splint made in a position that causes good movement of the sphenoid bone, temporal bone, and occipital bone of the skull and performs a MOBILITY TEST that examines the movement of the maxillary bone, sphenoid bone, and occipital bone, you can see that it moves well in a three-dimensional direction. Everything that I announce is a presentation that I feel directly with palpating.
https://progressinorthodontics.springeropen.com/.../s4051...
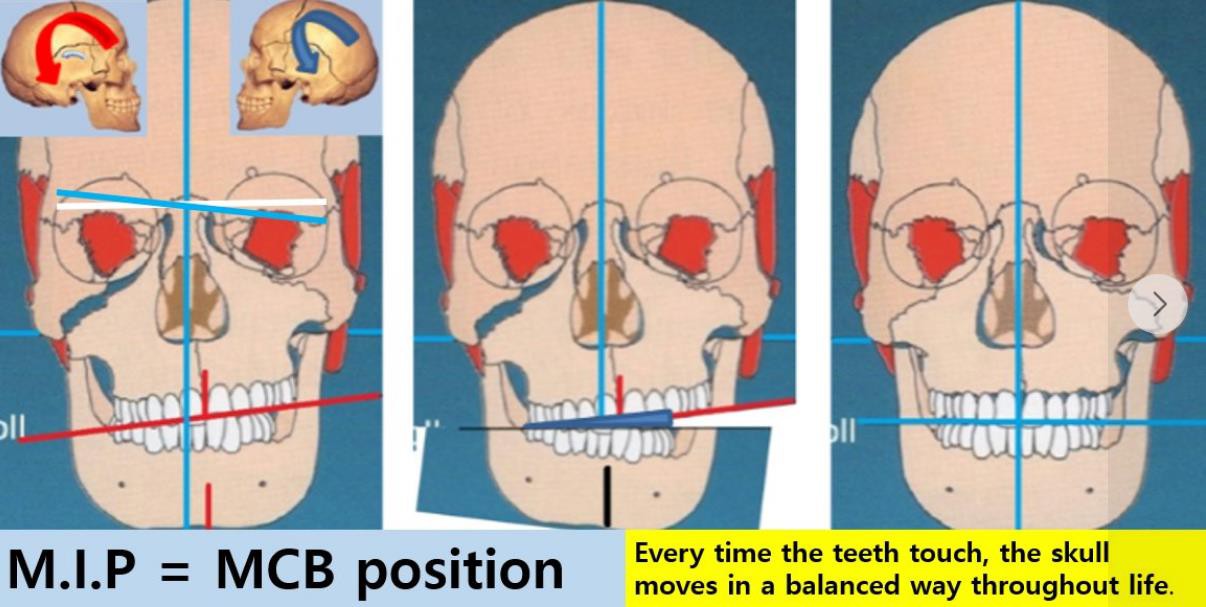
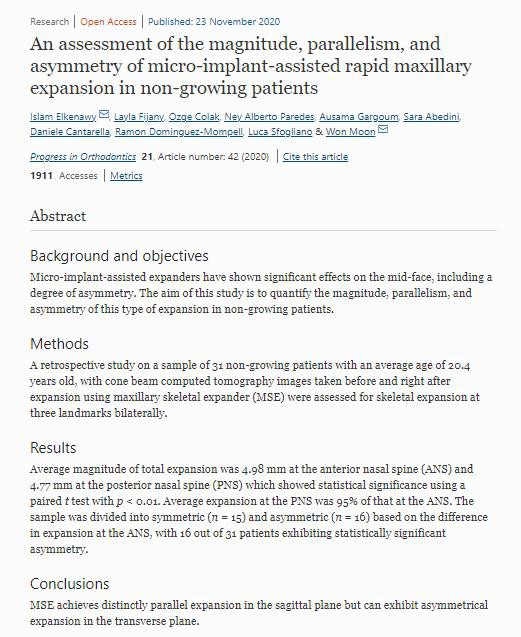
※ Extraction Orthodontics Reversal
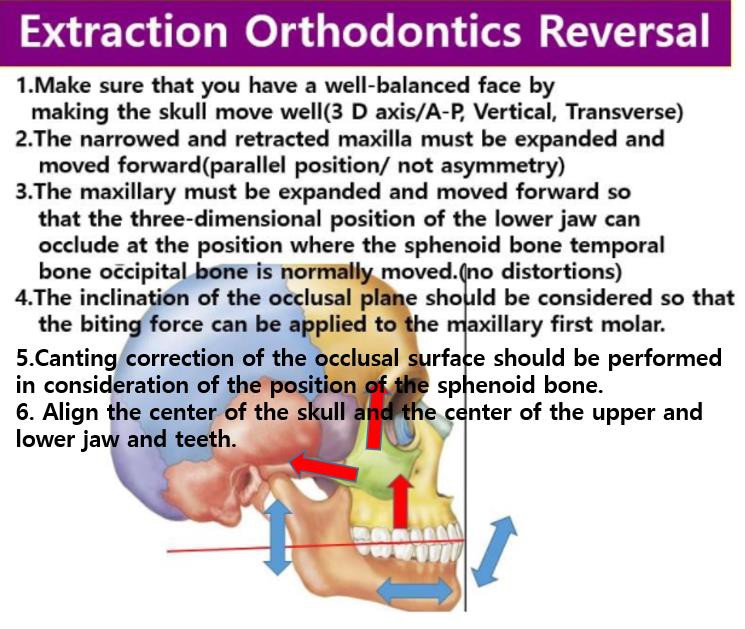
※ The root cause of vocal cord paralysis is an upper cervical vertebra.
The root cause of vocal cord paralysis is an upper cervical vertebra.
Cervicovagopathy
(C1/Occipital bone C2/Mandible /// Vagus nerve)
treated by MCB splint.
Signs and symptoms of vocal cord paralysis may include:
(Mayo Clinic)
A breathy quality to the voice
Hoarseness
Noisy breathing
Loss of vocal pitch
Choking or coughing while swallowing food, drink or saliva
The need to take frequent breaths while speaking
Inability to speak loudly
Loss of your gag reflex
Ineffective coughing
Frequent throat clearing
Causes
In vocal cord paralysis, the nerve impulses to your voice box (larynx) are disrupted, resulting in paralysis of the muscle. Doctors often don't know the cause of vocal cord paralysis. Known causes may include:
Injury to the vocal cord during surgery. Surgery on or near your neck or upper chest can result in damage to the nerves that serve your voice box. Surgeries that carry a risk of damage include surgeries to the thyroid or parathyroid glands, esophagus, neck, and chest.
Neck or chest injury. Trauma to your neck or chest may injure the nerves that serve your vocal cords or the voice box itself.
Stroke. A stroke interrupts blood flow in your brain and may damage the part of your brain that sends messages to the voice box.
Tumors. Tumors, both cancerous and noncancerous, can grow in or around the muscles, cartilage or nerves controlling the function of your voice box and can cause vocal cord paralysis.
Infections. Some infections, such as Lyme disease, Epstein-Barr virus and herpes, can cause inflammation and directly damage the nerves in the larynx.
Neurological conditions. If you have certain neurological conditions, such as multiple sclerosis or Parkinson's disease, you may experience vocal cord paralysis.
Complications
Breathing problems associated with vocal cord paralysis may be so mild that you just have a hoarse-sounding voice, or they can be so serious that they're life-threatening.
Because vocal cord paralysis keeps the opening to the airway from completely opening or closing, other complications may include choking on or actually inhaling (aspirating) food or liquid. Aspiration that leads to severe pneumonia is rare but serious and requires immediate medical care
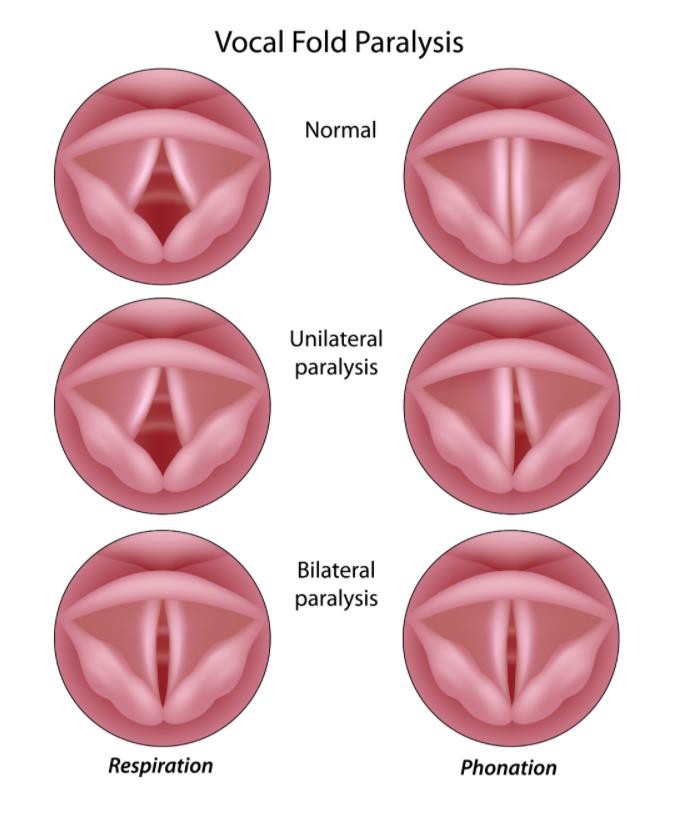
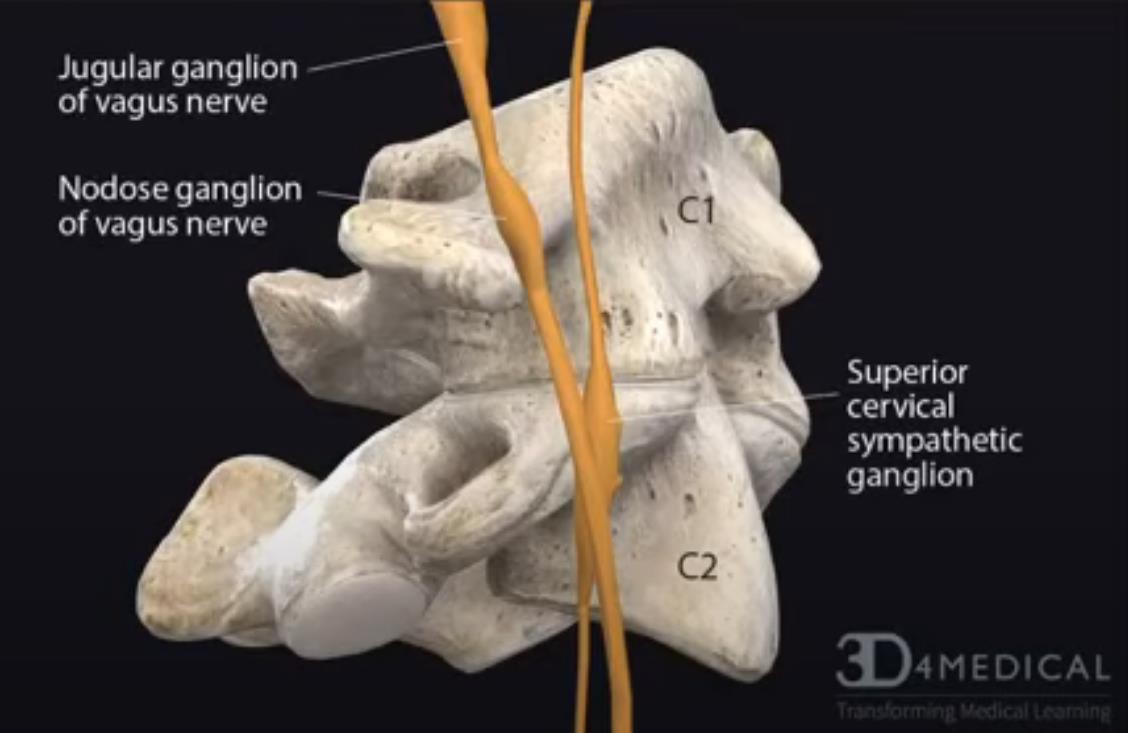
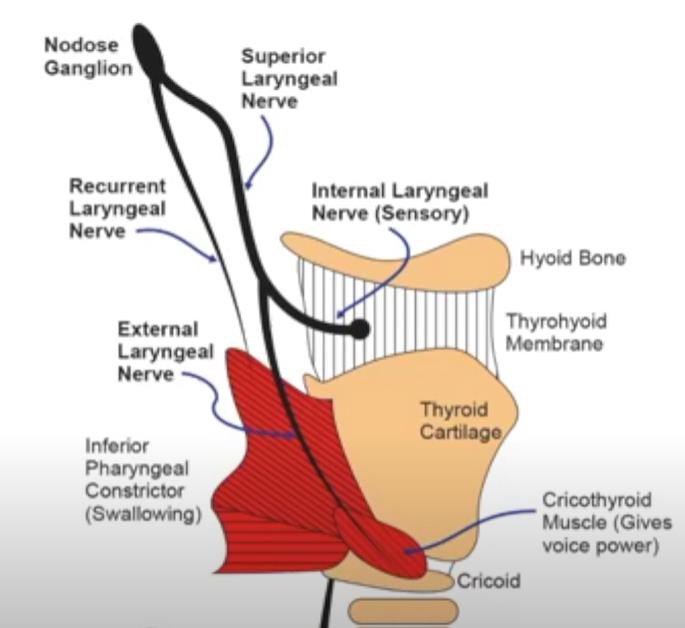
※ BRAIN FOG
Most people have an asymmetry in the skull. If the lower jaw is distorted in a three-dimensional position, the skull twists a little more each time the teeth touch. If you compare the force of separating the fingers when the teeth are in contact and when the teeth are not in contact after the thumb and index finger are in contact, your lower jaw is in a distorted state when it is easy to separate when the teeth are in contact. You keep spinning the bones of your skull every time you touch your teeth. This will last a lifetime. Eventually, it can affect brain function and nerves and cause many symptoms, such as brain fog. Useful treatments include ALF, cranial osteopathy, and mandibular skull balancing (MCB). MCB therapy instantly makes bilateral movement positive using a splint made in a position where the lower jaw enhances the movement of the skull. Brain function and nerves, jaw joints, facial asymmetry, and many other systemic symptoms are improved.
Kheng Hong Lau
If the mandible is asymmetry skeletally ie with one body or ramus longer than the other side, can we still align the mandible according to the idea of centrality, disregarding the position condylar head in the fossa? May i ask?
Jinhaeng Lee
Most people think that the difference between the left and right lengths of the jaw is different, but only if both lengths are the same, asymmetry is cured. If the skull is made of one bone, it will have to be adjusted by surgery. However, there are 22 skull bones, and the skull moves as if breathing, and while sleeping so that the body can function normally, it moves more actively. You cannot change the size or shape of each skull, but the position of the bones is constantly changing, so the face becomes more distorted. If you have a habit of sleeping on one side for a long time, you can think of asymmetry. The asymmetric prognathic retracting jaw treatment can be repositioned by using a method that increases the movement of the skull. The way to increase movement is to expand the maxilla and mandible.
When the maxilla is expanded using ALF, the teeth are slowly stretched, so even after 3 years of expansion, the amount of expansion or the movement of the skull does not increase much. So these days, MARPE is used for rapid expansion treatment to open the bone itself of the maxilla. Many connections in the skull are looser than before, so there is a lot of increased movement. In 2 months, you can expand as much as you want. But there is a problem. Most of the time there is asymmetry, so it will play faster and more than the amount that will be distorted with ALF or orthodontic treatment. So, if you expand using only MARPE/Rapid Expansion, it will twist the skull in 3D in a direction that is easy to move.
The way to prevent this is to do osteopathy treatment that increases the movement of the skull even further, and the movement occurs in the direction that it did not move. You need to do a lot of osteopathy treatment and see an osteopath who increases the movement of all 22 bones.
The MCB splint therapy is a way to increase the movement of the skull. If the lower jaw is in a distorted position, the skull will be twisted in three dimensions. However, a good left and right position of the lower jaw increases the movement of the sphenoid bone, and a good anteroposterior position of the lower jaw increases the movement of the temporal bone. A good height increases the movement of the occipital bone, so if it is used with MARPE, it can move in a non-moving direction, so asymmetry is treated. You can tell by the palpation of your fingers. At this time, if you use FACE MASK together, you can treat asymmetrical prognathic or retracting more quickly.

Changes in the movement of the skull after inoculation with the AZ vaccine.
First day.
My current skull movement shows the movements of our hospital patients wearing MCB/H. This movement is a state where flexion and extension movements appear quietly and slowly without distortion. I received the AZ corona vaccine on April 26, 2021 at 9:30 am. After that, there was no symptom of the skull movement until 6 pm, but as time passed, the skull started to twist. It was a symptom similar to the movement seen in patients with severe torticollis who was unable to control her head in the past. It's surprising. For me, this was the first time I had experienced this movement of my skull, so I was embarrassed. By 7:30 p.m., it was possible to promote the occurrence of the peak distortion. The movement around the pupils moved very badly, and I could feel the dazzling of the lights for the first time while driving when I left work. However, after 8 PM, the movement of the skull started to improve. And similar to usual, I went to sleep with MCB/L at 10:30 pm.
Second day
I couldn't get a deep sleep unlike usual. However, in the morning, the movement of the skull was as quiet as usual, and there were no other symptoms. However, around 6 pm, my skull was slightly twisted and I experienced a slight pain in the right sphenoid bone that lasted for about 30 minutes.
3rd day
I had a deep sleep as usual. The movement of my skull is as quiet as usual. Today is the day when the dental hospital is open until 9 pm. There was no problem with working. So I forgot to get vaccinated, drank a little hennessy in a glass of beer and slept.
4th day
Today is a day off for the dental hospital. My current state is the everyday serenity itself.
#mcbsplint
I became a journal editor.
https://voxcon.org/home/


Thank you Dr. Gerald H. Smith
My respected Master.
The MCB Splint comes from your teaching.
Dr. Smith's return to Korea was an over whelming success. Dr. Smith presented a two day seminar to an enthusiastic group of his previous students. On completion of the seminar, he reflected, "It was heart warming to hear that my concepts were being applied specially from the success stories from my students. As James Taylor said, 'The secret of life is enjoying the passage of time.' My 18 hours of travel time was worth every minute."
https://www.icnr.com/
MARPE(miniscrew-assisted rapid palatal expander)

nasal airway expansion(1-1A) and condyle density and shape(2-2A)

nasal airway(3-3A) and canting(4-4A) change
Only expansion!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!
NO!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!
BY
1. control expansion rate.
2. oneside screwing up.
3. Facial mask/ palpating sphenid bone, temporal bone and occipital bone.
4. Pivot splint / palpating sphenid bone, temporal bone and occipital bone.
5. MCB splint/ customize.
6. MCB splint/ disposable.


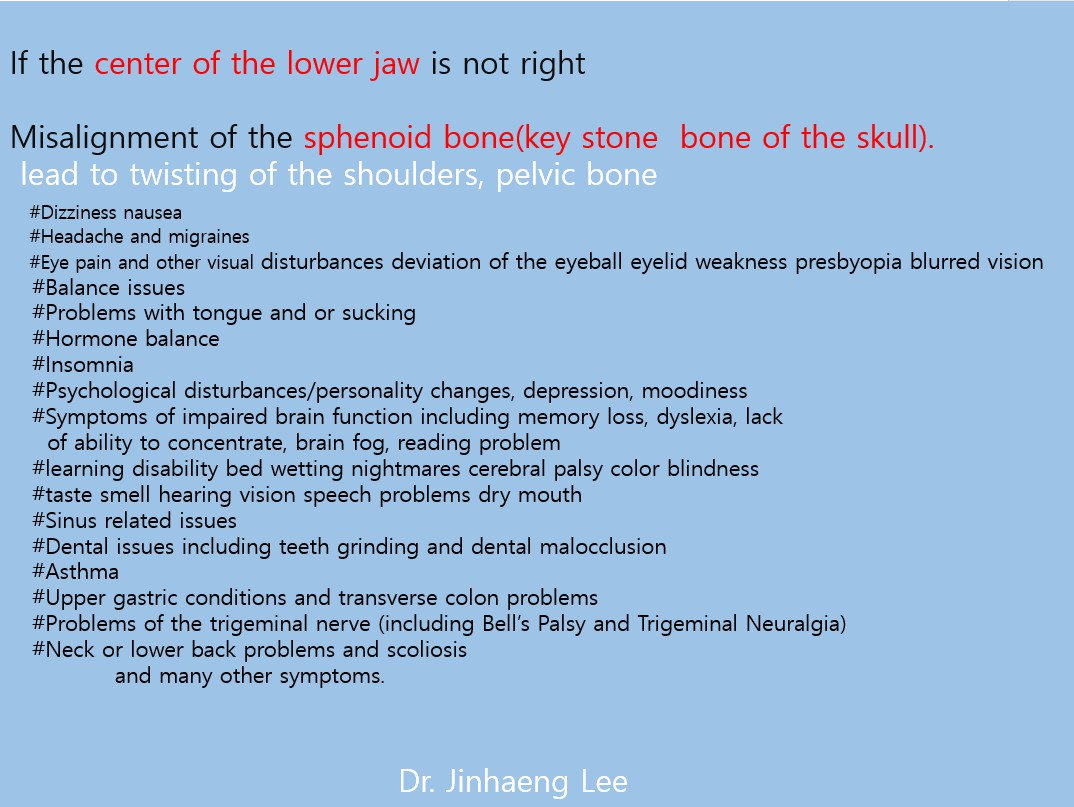
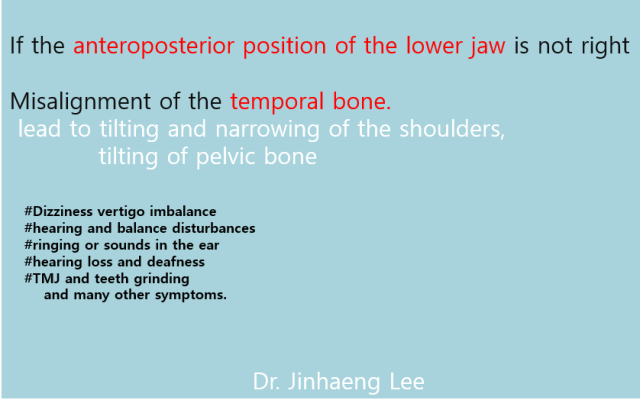


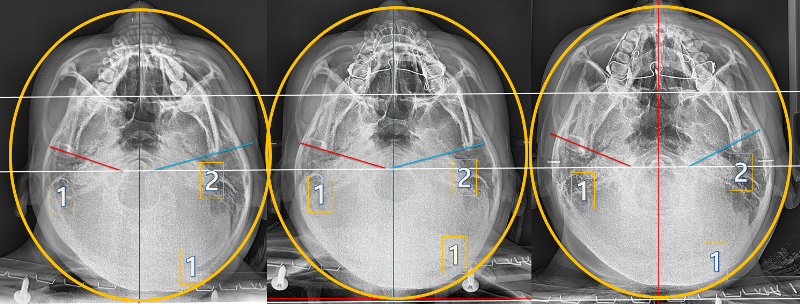
MCB treatment
1. cranial shape
2. Condyle assembly movement(angulation) and improvement of mandible asymmetry
3. Facial outline change and temperature of skull (below)
J Appl Oral Sci
. Sep-Oct 2012;20(5):526-30. doi: 10.1590/s1678-77572012000500006.
Histomorphometric Analysis of the Temporal Bone After Change of Direction of Force Vector of Mandible: An Experimental Study in Rabbits
Edela Puricelli 1, Deise Ponzoni, Jéssica Cerioli Munaretto, Adriana Corsetti, Mauro Gomes Trein Leite
Affiliations expand
PMID: 23138738 PMCID: PMC3881785 DOI: 10.1590/s1678-77572012000500006
Free PMC article
Abstract
Objectives: The present study aimed at performing a histological evaluation of the response of temporal bone tissue to a change of direction of the force vector of the mandible in relation to the base of the skull.
Material and methods: Adult rabbits were assigned into four groups with two control and four experimental animals in each group. experimental animals underwent surgery, which resulted in a change of direction of the force vector on the right temporomandibular joint. Samples were collected after 15, 30, 60 and 90 days for histological analysis.
Results: In the two-way analysis of variance, the effect of group and time was statistically significant (p<0.001). Additionally, a statistically significant interaction between group and time was observed (p<0.001). Control animals showed normal growth and development of the temporal region. In the experimental group, the change in direction of the force vector of the mandible induced significant changes in the temporal bone, with a bone modeling process, which suggests growth of this cranial structure.
Conclusions: The methodology used in this experiment allows us to conclude that the change in direction of the force vector of the mandible in relation to the skull base induces remodeling and modeling processes in the temporal bone. The resumption of normal oral functions after bone healing of the mandibular fracture appears to increase cell activation in the remodeling and modeling of the temporal bone structure. The observation of areas of temporal bone modeling shows the relevance of further investigation on the correlation between the joint structures and craniofacial growth and development.

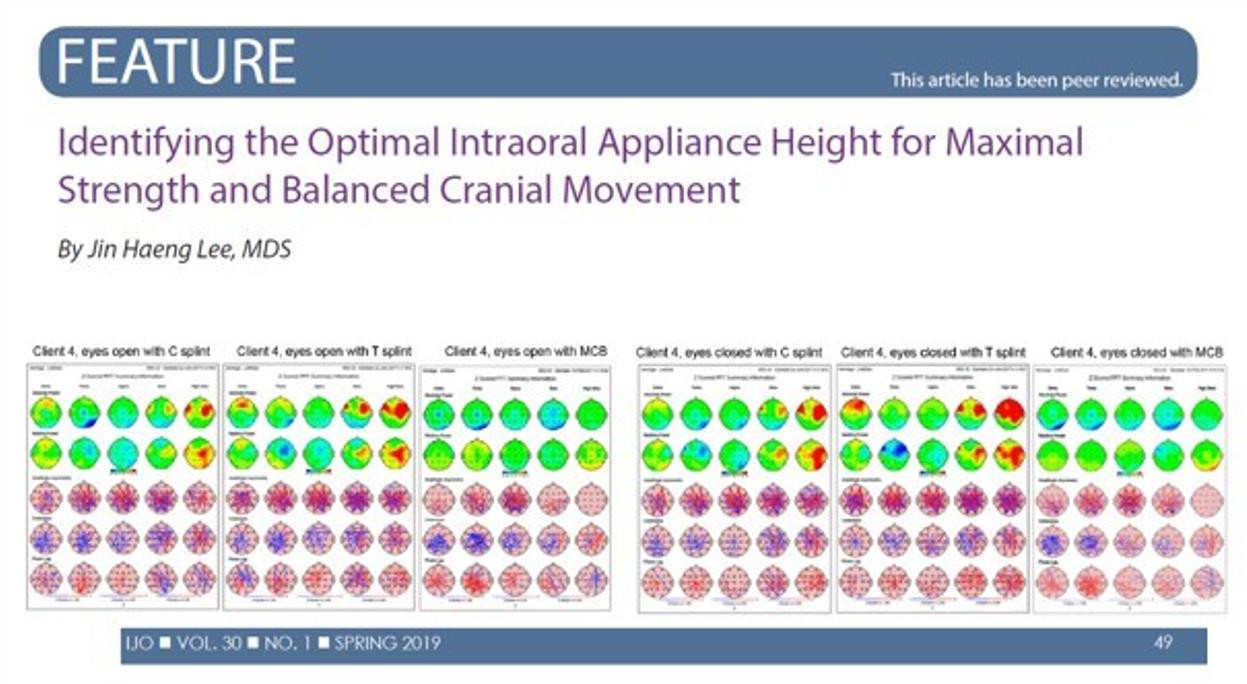

Following our Movement and Cognition conferences at Oxford University and at Harvard Medical School, we have the honor to invite you to the 2019 world conference on Movement and Cognition at Tel-Aviv University
Dear colleagues,
Following our Movement and Cognition conferences at Oxford University and at Harvard Medical School, we have the honor to invite you to the 2019 world conference on Movement and Cognitionat Tel-Aviv University.
The purpose of the conference is to share knowledge on the relation of human movement to cognitive function. Among the focus areas of the conference include applications for: Rehabilitation and therapeutics, sport, motor learning, brain-behavior relationships, gait and cognition, and dance. We are also focusing this time on female cognitive movement interaction, the aging brain and gerontology, treatment of traumatic brain injury, neonatal, infant and child development and ergonomics all in the context of movement and cognition.
The conference will be held on the campus of the University in the vibrant and fascinating city of Tel-Aviv between 22-24 July 2019. Besides the academic, scientific and clinical presentations, tours will also be available.
We welcome your participation in this conference. Should you, in addition, desire to present your research, unique technique or clinical experiences, kindly send us your abstract. This can be done by sending to the attention of the secretary of the scientific committee at: j*****@zahav.net.il. The abstracts of the conference will be published in the Conference Proceedings as well as selected papers published in volume 9 of the journal Functional Neurology, Rehabilitation, and Ergonomics
Dr. Jin Haeng Lee, Interested in Giving a Speech at World Convention of Aesthetic Medicine?
The 1st Annual World Convention of Aesthetic Medicine-2019
Time: Oct 11-13, 2019
Place: Dalian, China
Dear Dr. Jin Haeng Lee,
This is Miranda. Hope this email finds you well.
On behalf of the Organizing Committee, it is our delight to extend to you this Invitation to 1st Annual World Convention of Aesthetic Medicine-2019 which is going to be held during October 11-13, 2019 at Dalian, China. We sincerely invite you to attend this convention and deliver a talk in Stream 17 Oral Dental Caring Room ! If you are interested in attending WCAM, please send the talk title to me at your earliest.
Bookmark your dates for Dental Conferences 2019
Dear Dr. Jin Haeng Lee�,
Greetings!
We, from Coalesce research Group& The University of Georgia would like to have your presence as a Speaker or Delegate at the "Global Summit on Dentistry and Integrated Medicine" to be held on October 16-18, 2019 at The University of Georgia, Tbilisi, Georgia giving your views on the Theme "Future Vision of Dental and Oral Health Care"
Keynote Speaker Invitation at Future Dentistry 2019
Dear Dr. Jin Haeng Lee,
Greetings from Future Dentistry 2019.
The purpose of this letter is to invite you with honor to become an Keynote Speaker / Delegate for the upcoming Conference 25th American Dental Research & Future Dentistry which will be held during June 14-15, 2019 at Montreal, Canada
Invitation to Speak at Prosthodontics 2019
Dear Dr. Jin Haeng Lee,
In April 8-9, 2019 Conference series LLC is hosting 4th International Conference on Prosthodontics & Restorative Dentistry (Prosthodontics 2019), which will take place in the beautiful city Toronto, Canada. Since you have such great achievements in the field of Dentistry, we are glad to welcome you as a Speaker.
Your Research will have Immediate Global Impact - Dental 2018
Dear Dr.Jin Haeng Lee,
Greetings!
We take great pleasure in inviting you to the World Congress on Dental and Oral Health Conference. The conference is being held at Vancouver, CANADA from March 29th- 31st, 2018.
We are glad to invite Delegates, Students, Speakers, Poster Presenters, Organizing Committee Members (OCM), Moderators, Young researchers and Doctoral researchers. For more details regarding the conference, please review the descriptions on the website. It includes all of the details on the conference topics, professional development sessions, branding and promotions that are planned for these three days. I hope that you will attend many of these sessions, which will provide you to meet with professionals in your field
Dr.Jin Haeng Lee, Your Acknowledgement required towards American Dental Congress 2017
American Dental Congress 2017
September 18-20, 2017 Philadelphia, USA
"Exploring the possibilities in shaping the future of dental and oral health"
Meet world leading Dental & Healthcare professionals from 50 Countries & 5 Continents
Dear Dr.Jin Haeng Lee,
The purpose of this letter is to welcome you, to be a speaker at the upcoming "26th American Dental Congress" on September 18-20, 2017 Philadelphia, USA a leading forum for Dentists, Healthcare Physicians, Scientists, University faculty, Primary Healthcare and Community care Specialists, Public Health Specialists, Healthcare professional, to provide the ideal environment to disseminate and gain current knowledge in the area of Dental and Oral Health.
Effectiveness of Osteopathic Manipulative Treatment Versus Osteopathy in the Cranial Field in Temporomandibular Disorders - A Pilot Study
Christina Gesslbauer 1, Nadja Vavti 1, Mohammad Keilani 1, Michael Mickel 1, Richard Crevenna 1
Affiliations expand
PMID: 28029069 DOI: 10.1080/09638288.2016.1269368
Abstract
Purpose: Temporomandibular disorders are a common musculoskeletal condition causing severe pain, physical and psychological disability. The effect and evidence of osteopathic manipulative treatment and osteopathy in the cranial field is scarce and their use are controversial. The purpose of this pilot study was to evaluate the effectiveness of osteopathic manipulative treatment and osteopathy in the cranial field in temporomandibular disorders.
Methods: A randomized clinical trial in patients with temporomandibular disorders was performed. Forty female subjects with long-term temporomandibular disorders (>3 months) were included. At enrollment, subjects were randomly assigned into two groups: (1) osteopathic manipulative treatment group (20 female patients) and (2) osteopathy in the cranial field group (20 female patients). Examination was performed at baseline (E0) and at the end of the last treatment (E1), consisting of subjective pain intensity with the Visual Analog Scale, Helkimo Index and SF-36 Health Survey. Subjects had five treatments, once a week. 36 subjects completed the study (33.7 ± 10.3 y).
Results: Patients in both groups showed significant reduction in Visual Analog Scale score (osteopathic manipulative treatment group: p = 0.001; osteopathy in the cranial field group: p< 0.001), Helkimo Index (osteopathic manipulative treatment group: p = 0.02; osteopathy in the cranial field group: p = 0.003) and a significant improvement in the SF-36 Health Survey - subscale "Bodily Pain" (osteopathic manipulative treatment group: p = 0.04; osteopathy in the cranial field group: p = 0.007) after five treatments (E1). All subjects (n = 36) also showed significant improvements in the above named parameters after five treatments (E1): Visual Analog Scale score (p< 0.001), Helkimo Index (p< 0.001), SF-36 Health Survey - subscale "Bodily Pain" (p = 0.001). The differences between the two groups were not statistically significant for any of the three target parameters.
Conclusion: Both therapeutic modalities had similar clinical results. The findings of this pilot trial support the use of osteopathic manipulative treatment and osteopathy in the cranial field as an effective treatment modality in patients with temporomandibular disorders. The positive results in both treatment groups should encourage further research on osteopathic manipulative treatment and osteopathy in the cranial field and support the importance of an interdisciplinary collaboration in patients with temporomandibular disorders. Implications for rehabilitation Temporomandibular disorders are the second most prevalent musculoskeletal condition with a negative impact on physical and psychological factors. There are a variety of options to treat temporomandibular disorders. This pilot study demonstrates the reduction of pain, the improvement of temporomandibular joint dysfunction and the positive impact on quality of life after osteopathic manipulative treatment and osteopathy in the cranial field. Our findings support the use of osteopathic manipulative treatment and osteopathy in the cranial field and should encourage further research on osteopathic manipulative treatment and osteopathy in the cranial field in patients with temporomandibular disorders. Rehabilitation experts should consider osteopathic manipulative treatment and osteopathy in the cranial field as a beneficial treatment option for temporomandibular disorders.
Keywords: Temporomandibular joint; osteopathic medicine; pain; pain management.
Comparative Study Cranio
. 2010 Oct;28(4):266-73. doi: 10.1179/crn.2010.034.
Immediate Effect of the Resilient Splint Evaluated Using Surface Electromyography in Patients With TMD
André Luís Botelho 1, Bruno Caetano Silva, Flávio Henrique Umeda Gentil, Chiarella Sforza, Marco Antonio Moreira Rodrigues da Silva
Affiliations expand
PMID: 21032981 DOI: 10.1179/crn.2010.034
Abstract
The aim of this study was to analyze the immediate effect of resilient splints through surface electromyography testing and to compare the findings with the electromyographic profiles of asymptomatic subjects. The participants were 30 subjects, 15 patients with TMD (TMD Group) and 15 healthy subjects (Control Group), classified according to Research Diagnostic Criteria (RDC/TMD) Axis I. A resilient occlusal splint was made for each patient in the TMD Group from two mm thick silicon to cover all teeth. The EMG examination was performed before and immediately after installing the splint. Three tests were performed as follows: 1. Maximum Voluntary Contraction (MVC) using cotton rolls (standards test); 2. MVC in maximal intercuspation position; and 3. MVC with the splint in position. The EMG signal was recorded for five seconds. EMG indices were calculated to assess muscle symmetry, jaw torque, and impact. There was a statistically significant difference when comparing the results among the study groups. The symmetry index values in the Control Group were higher than the TMD Initial Group and similar to the TMD Group after the installation of the splint. The index values of torque were higher in TMD Initial Group when compared with the Controls. Impact values were lower than normal values in the TMD Initial Group and restored upon installation of the splint. The resilient occlusal splints may be used as complementary or adjunctive treatment of temporomandibular disorders.
Cranio
. 2011 Jul;29(3):178-86. doi: 10.1179/crn.2011.026.
Bruxism and Temporal Bone Hypermobility in Patients With Multiple Sclerosis
David E Williams 1, John E Lynch, Vidhi Doshi, G Dave Singh, Alan R Hargens
Affiliations expand
PMID: 22586826 DOI: 10.1179/crn.2011.026
Abstract
In this study, the authors investigated the link between jaw clenching/bruxism and temporal bone movement associated with multiple sclerosis (MS). Twenty-one subjects participated in this study (10 patients with MS and 11 controls). To quantify the change in intracranial dimension between the endocranial surfaces of the temporal bones during jaw clenching, an ultrasonic pulsed phase locked loop (PPLL) device was used. A sustained jaw clenching force of 100 lbs was used to measure the mean change in acoustic pathlength (delta L) as the measure of intracranial distance. In the control subjects the mean delta L was 0.27 mm +/- 0.24. In subjects with MS the mean delta L was 1.71 mm +/- 1.18 (p<0.001). The increase in magnitude of bi-temporal bone intracranial expansion was approximately six times greater in subjects with MS compared to controls. Therefore, jaw clenching/bruxism is associated with more marked displacement of the temporal bones and expansion of the cranial cavity in patients with MS than in control subjects.
Hum Brain Mapp
. 2012 Dec;33(12):2984-93. doi: 10.1002/hbm.21466. Epub 2011 Nov 18.
The Cerebral Representation of Temporomandibular Joint Occlusion and Its Alternation by Occlusal Splints
Martin Lotze 1, Christian Lucas, Martin Domin, Bernd Kordass
Affiliations expand
PMID: 22102437 DOI: 10.1002/hbm.21466
Abstract
Occlusal splints are a common and effective therapy for temporomandibular joint disorder. Latest hypotheses on the impact of occlusal splints suggest an altered cerebral control on the occlusion movements after using a splint. However, the impact of using a splint during chewing on its cerebral representation is quite unknown. We used functional magnetic resonance imaging (fMRI) to investigate brain activities during occlusal function in centric occlusion on natural teeth or on occlusal splints in fifteen healthy subjects. Comparisons between conditions revealed an increased activation for the bilateral occlusion without a splint in bilateral primary and secondary sensorimotor areas, the putamen, inferior parietal and prefrontal cortex (left dorsal and bilateral orbital) and anterior insular. In contrast, using a splint increased activation in the bilateral prefrontal lobe (bilateral BA 10), bilateral temporo-parietal (BA 39), occipital and cerebellar hemispheres. An additionally applied individually based evaluation of representation sites in regions of interest demonstrated that the somatotopic representation for both conditions in the pre- and postcentral gyri did not significantly differ. Furthermore, this analysis confirmed the decreasing effect of the splint on bilateral primary and secondary motor and somatosensory cortical activation. In contrast to the decreasing effect on sensorimotor areas, an increased level of activity in the fronto-parieto-occipital and cerebellar network might be associated with the therapeutic effect of occlusal splints.
Touch—More Than a Basic Science
Mitchell L. Elkiss, DO; John A. Jerome, PhD
Author Notes
The Journal of the American Osteopathic Association, August 2012, Vol. 112, 514-517.
Abstract
The potency of touch in osteopathic manipulative treatment (OMT) is physically realized within the musculoskeletal, immune, nervous, and endocrine systems. Psychologically, touch supports a verbal and tactile interaction that is both diagnostic and therapeutic. Touch is a 2-way street that adds meaning and depth to the patient-physician experience. The relationship between touching and being touched offers a potentially powerful and intense deepening of the patient-physician relationship that emerges within the palpatory examination and treatment. Empathic communication, through word or deed, allows a therapeutic, synchronized healing to occur. In the present article, the authors provide a rationale to sensitize and invigorate osteopathic physicians to routinely evaluate and treat patients using their skillful touch.
Figure 1.
The musculoskeletal, immune, nervous, and endocrine (MINE) systems interact in response to low-threshold mechanical stimulation, which is perceived as touch, and to nociceptive input, which is perceived as pain. Dysregulation in the MINE systems, expressed through the musculoskeletal system as somatic dysfunction, can be diagnosed during palpatory examination. Reprinted with permission from Lippincott Williams & Wilkins.15

Asymmetric nasomaxillary expansion induced by tooth‐bone‐borne expander producing differential craniofacial changes
Kyung‐A Kim Song‐Hee Oh Byoung‐Ho Kim Su‐Jung Kim
First published:07 May 2019 https://doi.org/10.1111/ocr.12320
Read the full text
PDFPDFTOOLS SHARE
Abstract
Objectives
To evaluate three‐dimensional (3D) craniofacial changes induced by a non‐surgical tooth‐bone‐borne rapid palatal expander (TBB‐RPE) according to the symmetrical pattern of expansion, to investigate the 3D changes between the sides in patients with asymmetric expansion, and to identify the related factors of asymmetric expansion.
Setting and sample population
Sixty‐six patients (mean age: 19.3 ± 5.7 years) treated with TBB‐RPE were divided into a symmetric expansion group (Group S, n = 46) or asymmetric expansion group (Group A, n = 20). Group S was subdivided into Group Ss (n = 27), with bilateral frontomaxillary suture (FMS) split, and Group Sn (n = 19), with no FMS split.
Materials and methods
Pre‐ and post‐expansion cone‐beam computed tomography images were superimposed, and the common coordinated system was set. All landmarks were designated as coordinate pairs, and treatment changes were automatically calculated. Analysis of variance was conducted for intergroup comparison of craniofacial changes, and logistic regression analysis was performed to identify the related factors of asymmetric expansion.
Results
The frequency of asymmetric expansion was 30.3%. Group A with unilateral FMS split showed less craniofacial changes than Group Ss and more changes than Group Sn. Group A exhibited different nasomaxillary displacement between the two halves, showing greater changes in the FMS‐split side. Among the tested six variables (age, gender, Angle's classification, unilateral crossbite, maxillary cant and chin deviation), chin deviation was uniquely associated with asymmetric expansion.
Conclusions
Tooth‐bone‐borne rapid palatal expander had a risk of asymmetric expansion, especially in facial asymmetric patients with chin deviation, producing different craniofacial changes from symmetric expansion.
Eur J Radiol
. 2004 Sep;51(3):269-73. doi: 10.1016/S0720-048X(03)00218-3.
Relationship of Condylar Position to Disc Position and Morphology
L Incesu 1, N Taşkaya-Yilmaz, M Oğütcen-Toller, E Uzun
Affiliations expand
PMID: 15294336 DOI: 10.1016/S0720-048X(03)00218-3
Abstract
Introduction/objective: The purpose of this study was to assess whether condylar position, as depicted by magnetic resonance imaging, was an indicator of disc morphology and position.
Methods and material: One hundred and twenty two TMJs of 61 patients with temporomandibular joint disorder were examined. Condylar position, disc deformity and degree of anterior disc displacement were evaluated by using magnetic resonance imaging.
Results and discussion: Posterior condyle position was found to be the main feature of temporomandibular joints with slight and moderate anterior disc displacement. No statistical significance was found between the condylar position, and reducing and nonreducing disc positions. On the other hand, superior disc position was found to be statistically significant for centric condylar position.
Conclusion: It was concluded that posterior condyle position could indicate anterior disc displacement whereas there was no relation between the position of condyle and the disc deformity.
https://www.westonaprice.org/health-topics/dentistry/is-it-mental-or-is-it-dental/#.XLPlztQE_c5.email
#tmjd #tmj disc #tmj click #lockjaw #tmj pain #nonsurgical facial asymmetry #tic disorder #tourette syndrome #dystonia #torticollis #trigeminal neuralgia #wryneck #parkinson’s disease #disc #headache #autoimmune disease #fibromyalgia #sleep apnea #dizziness #vertigo #migrain #watery eye #astigmatism #ringing the ear #tinnitus #otitis #mastoiditis #allergy #meniere's disease #proprioceptive dysfunctions #ataxia #labyrinthitis #condilo arthrosis #ATM dysfunctions #trigeminal pain #nasal breathing obstruction #sinusitis #asthma #obstructive apnea #mouth breathing #phonatory problems #swallowing problems #lump in the throat feeli
제목을 입력하시려면 더블클릭하세요.
단락을 입력하시려면 더블클릭하세요.
단락은 좀더 자세한 내용을 넣어 사용자들에게 정보를 쉽게 전달할 수 있습니다.